Armamentarium
|
Indications for Removal of Impacted Third Molars
The parameters of care published by the American Association of Oral and Maxillofacial Surgeons have established criteria for the extraction of impacted third molars. The indications for removal of impacted third molars include:
- 1.
Pain
- 2.
Pathology associated with tooth follicle (e.g., cysts, tumors)
- 3.
Abnormalities of tooth size or shape that preclude normal function
- 4.
Facilitation of the management or limitation of progression of periodontal disease
- 5.
Resorption of third molar or adjacent tooth
- 6.
Facilitation of orthodontic tooth movement and promotion of stability of the dental occlusion
- 7.
Facilitation of prosthetic rehabilitation
- 8.
Tooth impeding the normal eruption of an adjacent tooth
- 9.
Tooth in the line of fracture
- 10.
Tooth involved in tumor resection
- 11.
Tooth interfering with orthognathic and/or reconstructive jaw surgery
- 12.
Preventive or prophylactic tooth removal, when indicated, for patients with medical or surgical conditions or treatments (e.g., organ transplants, alloplastic implants, antiresorptive therapy, chemotherapy, radiation therapy)
- 13.
Clinical findings of fractured tooth or teeth
- 14.
Facilitation of harvesting of autologous graft
- 15.
Impacted tooth (as defined previously)
- 16.
Anatomic position causing potential damage to adjacent teeth
- 17.
Patient’s informed refusal of nonsurgical treatment options
Diagnostic Imaging
A panoramic radiograph is recommended for management of third molars, although periapical, maxillary, and/or mandibular radiographs and computed tomography may also be used. The goals of impacted tooth removal are to:
- •
Prevent pathology
- •
Preserve the periodontal health of adjacent teeth
- •
Optimize prosthetic rehabilitation
- •
Optimize management and/or healing of jaw fractures
- •
Optimize orthodontic results
- •
Aid in tumor resection
- •
Provide a healthy oral and maxillofacial environment for patients undergoing radiation therapy, chemotherapy, organ transplantation, or placement of alloplastic implants
- •
Prevent complications in orthognathic surgery
Indications for Removal of Impacted Third Molars
The parameters of care published by the American Association of Oral and Maxillofacial Surgeons have established criteria for the extraction of impacted third molars. The indications for removal of impacted third molars include:
- 1.
Pain
- 2.
Pathology associated with tooth follicle (e.g., cysts, tumors)
- 3.
Abnormalities of tooth size or shape that preclude normal function
- 4.
Facilitation of the management or limitation of progression of periodontal disease
- 5.
Resorption of third molar or adjacent tooth
- 6.
Facilitation of orthodontic tooth movement and promotion of stability of the dental occlusion
- 7.
Facilitation of prosthetic rehabilitation
- 8.
Tooth impeding the normal eruption of an adjacent tooth
- 9.
Tooth in the line of fracture
- 10.
Tooth involved in tumor resection
- 11.
Tooth interfering with orthognathic and/or reconstructive jaw surgery
- 12.
Preventive or prophylactic tooth removal, when indicated, for patients with medical or surgical conditions or treatments (e.g., organ transplants, alloplastic implants, antiresorptive therapy, chemotherapy, radiation therapy)
- 13.
Clinical findings of fractured tooth or teeth
- 14.
Facilitation of harvesting of autologous graft
- 15.
Impacted tooth (as defined previously)
- 16.
Anatomic position causing potential damage to adjacent teeth
- 17.
Patient’s informed refusal of nonsurgical treatment options
Diagnostic Imaging
A panoramic radiograph is recommended for management of third molars, although periapical, maxillary, and/or mandibular radiographs and computed tomography may also be used. The goals of impacted tooth removal are to:
- •
Prevent pathology
- •
Preserve the periodontal health of adjacent teeth
- •
Optimize prosthetic rehabilitation
- •
Optimize management and/or healing of jaw fractures
- •
Optimize orthodontic results
- •
Aid in tumor resection
- •
Provide a healthy oral and maxillofacial environment for patients undergoing radiation therapy, chemotherapy, organ transplantation, or placement of alloplastic implants
- •
Prevent complications in orthognathic surgery
Contraindications to Removal of Impacted Third Molars
The surgeon should consider three important clinical factors in deciding whether to extract an impacted third molar :
- •
Patient of older age
- •
Compromised medical status
- •
Increased risk of damage to anatomic structures
Many classification systems correlate descriptive features of the tooth to the degree of difficulty in surgical extraction. The most common system, the Pell and Gregory classification ( Figure 11-1 ), incorporates the following features:
- 1.
The relationship of the impacted tooth to the anterior border of the ramus and the second molar
- 2.
The depth of the impaction and the type of tissue overlying the impacted tooth
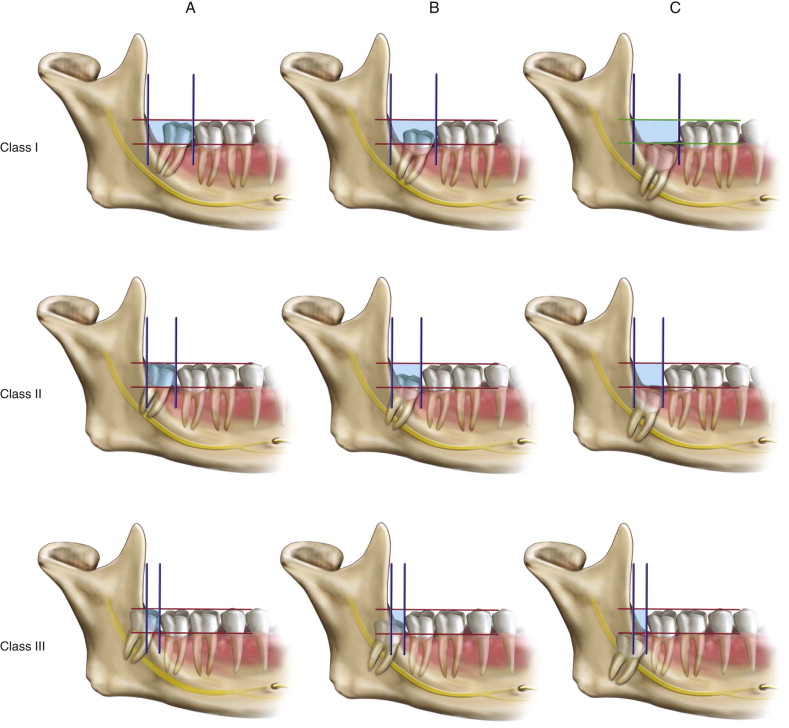
A third and more commonly used description is the angulation of the impacted tooth (horizontal, vertical, mesioangular, or distoangular).
Technique: Surgical Removal of Impacted Third Molars
Addressing the surgical removal of impacted teeth begins with access. Before a tooth can be extracted, clinically visualizing the surgical site is crucial. An envelope flap is most commonly used by surgeons in both the maxilla and mandible. The following considerations should be addressed when designing a surgical flap:
- •
Allow for complete visualization of the operative field.
- •
Prevent unnecessary trauma to the adjacent soft tissue when removing bone or teeth.
- •
Provide an adequate working area that allows for full removal of intrabony pathologic conditions when present.
- •
Place incisions over bone not planned for removal.
- •
Make sure the incision is long enough to allow for a flap that gives clear and adequate hard tissue visualization and permits easy retraction without tearing.
- •
Make sure the base of the flap is wider than the reflected free margin to ensure a proper blood supply to the reflected soft tissue.
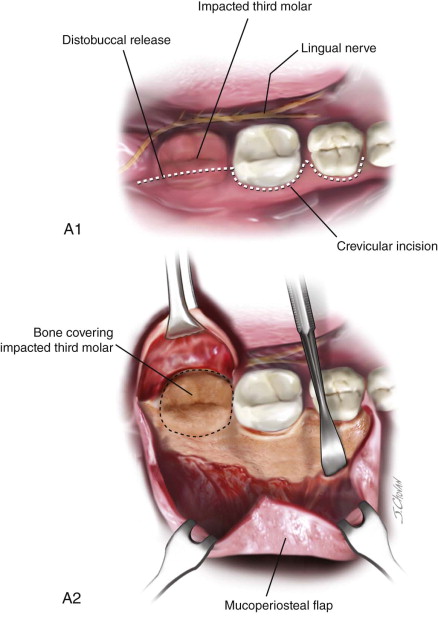
Step 1A:
Mandibular Incision
A sulcular incision is made from the distal of the first molar posteriorly with a distobuccal release in the mandible with an option to include a possible mesial vertical release for increased access ( Figure 11-2, A ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


