Armamentarium
|
History of the Procedure
The original description of the bilateral sagittal split osteotomy (BSSO) is credited to Trauner and Obwegeser. Although there have been many modifications designed to improve the procedure, two of the earlier ones were suggested by Hunsuck and Dal Pont. These two combined modifications have established the basic osteotomy as a procedure in which the bone cut on the medial aspect of the mandible stops at the lingual fossa and on the lateral extends forward along the external oblique ridge. Among the many additional authors who have suggested changes to the basic design is Epker, who in 1977 published a paper showing several modifications and emphasizing the need to maintain the blood supply to the proximal segment. Increased stability and early mobilization of the patient after a BSSO were introduced when Spiessl demonstrated that three 2.7-mm bicortical screws could be used to fix the proximal and distal segments. Since his publication in 1988, many alternatives have been used in the application of screws and/or plates to fix the segments. Most of these modifications have illustrated the use of smaller systems used to achieve early function and stability. Today the bilateral sagittal split, in its multiple iterations, is the most commonly used osteotomy for moving the mandible. The most frequent variations concern the length and design of the osteotomy on the proximal segment and the type of fixation used.
History of the Procedure
The original description of the bilateral sagittal split osteotomy (BSSO) is credited to Trauner and Obwegeser. Although there have been many modifications designed to improve the procedure, two of the earlier ones were suggested by Hunsuck and Dal Pont. These two combined modifications have established the basic osteotomy as a procedure in which the bone cut on the medial aspect of the mandible stops at the lingual fossa and on the lateral extends forward along the external oblique ridge. Among the many additional authors who have suggested changes to the basic design is Epker, who in 1977 published a paper showing several modifications and emphasizing the need to maintain the blood supply to the proximal segment. Increased stability and early mobilization of the patient after a BSSO were introduced when Spiessl demonstrated that three 2.7-mm bicortical screws could be used to fix the proximal and distal segments. Since his publication in 1988, many alternatives have been used in the application of screws and/or plates to fix the segments. Most of these modifications have illustrated the use of smaller systems used to achieve early function and stability. Today the bilateral sagittal split, in its multiple iterations, is the most commonly used osteotomy for moving the mandible. The most frequent variations concern the length and design of the osteotomy on the proximal segment and the type of fixation used.
Indications for the Use of the Procedure
The bilateral sagittal split is an extremely versatile procedure that can be used to advance the mandible, set it back, or correct asymmetry. Controversy exists over its use to close open bites. Several groups have shown that closing an open bite with mandibular advancement (counterclockwise movement) is less stable than clockwise advancement. Others have shown that although closing an open bite reduces stability, in selected instances it can be used.
The timing of third molar removal also is controversial. Several authors have suggested that they be removed 6 to 9 months before a bilateral sagittal split is performed to reduce the incidence of “bad” splits. Others have stated that the third molars can be taken out at the time of the surgery with minimal risk to the surgical outcome. It is clear that taking out the third molars at the time of the sagittal split takes a little longer and also that many factors contribute to “bad” splits; the presence of third molars is only one of them. Whether the third molars should be removed before surgery depends on a number of factors and the surgeon’s experience.
Limitations and Contraindications
As noted previously, there are several areas of controversy regarding the use of a bilateral sagittal split osteotomy. These include its use to close an open bite and whether third molars should be taken out before or at the time of the procedure. There is a higher incidence of inferior alveolar nerve injury with a bilateral sagittal split osteotomy than with a vertical ramus osteotomy when used to set back the mandible. However, a bilateral sagittal split can be more consistently fixed with plates and screws and hence allows the patient earlier function. Additional areas of controversy and limitations have to do with large advancements or setbacks. The mandible can be advanced 10 mm in most cases, and in many cases further movement can be achieved, depending on the anatomy of the patient. However, at some point, other procedures should be used to advance the mandible, such as an extraoral osteotomy, using bone grafts or distraction, to lengthen the mandible gradually.
For large advancements that can be achieved with a sagittal split, different strategies can be used to optimize bone overlap and stability. These include extending the Dal Pont modification a little farther forward and using more rigid forms of stabilization for the osteotomy. A period of intermaxillary fixation with skeletal stabilization in the form of circumferential wires has proved successful when large advancements were done. How much the mandible can be advanced with a BSSO depends on the surgeon’s background and the individual case.
Large setbacks with a bilateral sagittal split are unstable. The more the mandible is set back, the more it tends to come forward in the postoperative period. This instability or relapse may be due numerous factors. Although different osteotomy designs or fixation strategies can be used, in general, if a large setback is required to achieve an ideal occlusal result, a component of maxillary hypoplasia usually is present. As such, the patient would have a more stable and better esthetic result with two-jaw surgery.
Technique: Bilateral Sagittal Split to Advance the Mandible
Step 1:
Incision
With a mouth prop in place on the opposite side, a Minnesota retractor is placed just lateral to the external oblique ridge. With a needle point bovie electrocautery, an incision is made directly over the external oblique ridge at approximately the level of the occlusion and then extended inferior and lateral to the teeth, leaving a 5- to 6-mm gingival cuff ( Figure 33-1, A ).



Step 2:
Dissection
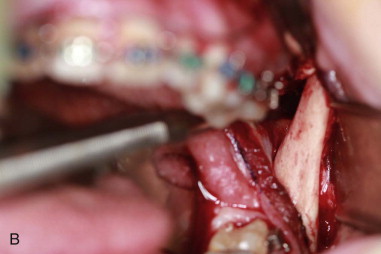
Elevate the mucosa and connective tissue enough to expose the external oblique ridge and place a coronoid notch retractor. Release the tissues in a subperiosteal plan to the tip of the coronoid process. Place a curved Kocher clamp with umbilical tape tied to it at the tip of the coronoid and secure it to the drape. Elevate the tissue along the medical aspect of the mandible to expose the lingual fossa ( Figure 33-1, B ).
Step 3:
Medial Osteotomy
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


