Armamentarium
|
History of the Procedure
Since the introduction of osseointegrated dental implants in Europe in the 1960s and in North America in the 1980s, dental implants have enjoyed phenomenal success. However, in the past decade, it has become evident that the same periodontal disease processes that affect teeth affect dental implants.
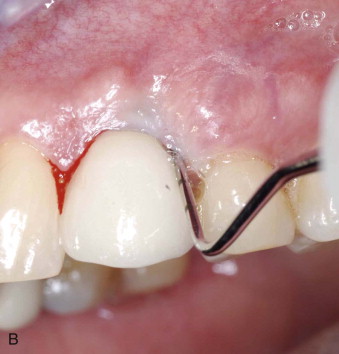
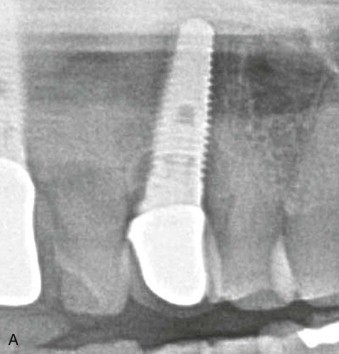
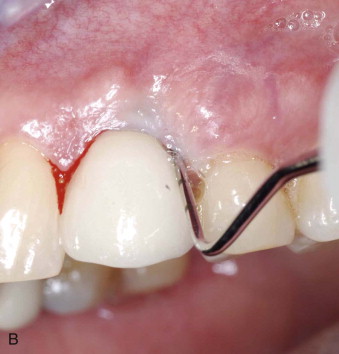
Peri-implantitis is defined as an inflammatory process affecting the tissues around an osseointegrated implant that results in loss of the supporting alveolar bone. Clinically it is present when three conditions are seen: radiographic evidence of bone loss exceeding the typical anatomic remodeling, pocket depths greater than 5 mm, and bleeding or suppuration on probing ( Figure 25-1, A and B ). The precursor to peri-implantitis is termed peri-implant mucositis ( Figure 25-1, C ), which is basically peri-implantitis without concomitant bone loss and which may be reversible with proper treatment. It is estimated that after 5 years, nearly 50% of implant sites may develop peri-implant mucositis. Peri-implant mucositis typically is treated nonsurgically, with curettage, chlorhexidine mouth rinse, and antibiotics.


Procedures to salvage dental implants are evolving. A study by Roos-Jansaker et al. in 2006 revealed a 12% incidence of peri-implantitis after 10 years in a European population. Recent studies have confirmed the undeniable prevalence of this problem. In a review of the epidemiology of peri-implantitis, Mombelli et al. stated that the prevalence of peri-implantitis is on the order of 10% of implants and 20% of patients after 5 to 10 years. Most studies also conclude that smoking and a history of periodontitis significantly affect a patient’s predisposition to developing peri-implantitis.
Peri-implantitis results in the loss of supporting bone and soft tissue. Treatment may involve removal of the implant (deplantation), débridement procedures, and regenerative procedures in conjunction with débridement. In the 1990s and early in the 2000s, many of the studies on peri-implantitis were done in the canine model using ligature-induced peri-implantitis. However, over the past decade, enough implants have been placed in the general population to allow studies using implants in patients.
It has been shown that reosseointegration can occur on a repaired surface. Reintegration may consist of soft tissue reattachment, osseous reattachment, or a combination of the two. Protocols for regenerative procedures are evolving; they include the use of allogeneic bone graft materials, autogenous bone graft materials, and commercially available tissue engineering products, such as recombinant human bone morphogenic protein (rhBMP) and recombinant platelet-derived growth factor (rhPDGF). Success rates vary, depending on the anatomy and amount of preexisting bone loss, but typically are in the 60% to 70% range. When an ideal repair situation exists, success rates approach 100%. In 2012 Heitz-Mayfield et al. reported a 47% elimination of bleeding on probing and a 92% level of resolution of bone loss after 12 months of antiinfective treatment combined with open débridement.
The etiology of peri-implantitis is multifactorial. One of the most common causes is retained cement from cementation of a prosthesis. If inflammation develops within weeks or months after crown cementation, surgical exploration for retained cement is indicated ( Figure 25-2 ).

Another common cause is periodontally compromised teeth elsewhere in the mouth. Studies have shown that pocket depths of 6 mm or more around teeth cause the seeding of implants with periodontal pathogens; peri-implantitis presents itself with a lag time of approximately 2 to 3 years after pocket development. Considerable research is under way regarding a genetic component underlying the individual susceptibility to implant loss. The interleukin-1 and interleukin-6 genes have been studied and may offer an explanation for the clusterization phenomenon, in which certain individuals appear to be susceptible to chronic periodontitis and peri-implantitis, resulting in an increased incidence of implant loss.
Other common causative factors include a poor prosthesis design that inhibits hygiene, inadequate attached tissue, endodontic defects on adjacent teeth, and systemic issues, such as smoking and diabetes. These issues need to be addressed and eliminated, when possible, before the repair is undertaken.
It is interesting to note that when Brånemark and colleagues originally presented their 15-year success rates, their long-term success rates were high, and peri-implantitis was not a major problem in their patient population. This is likely due to the fact that the vast majority of their original patients were edentulous and had screw-retained prostheses. Their protocol thereby eliminated the two most common causes of peri-implantitis: retained cement and periodontal pathogens associated with periodontally compromised natural teeth.
Prevention of peri-implantitis starts with proper implant site development, obtaining optimized bone and soft tissue, and subsequent ideal implant placement. Prevention of periodontal disease elsewhere in the mouth, proper prosthesis design for adequate hygiene, prevention of retained cement, and regular hygiene recall for early detection of peri-implantitis are all necessary to minimize peri-implant disease.
History of the Procedure
Since the introduction of osseointegrated dental implants in Europe in the 1960s and in North America in the 1980s, dental implants have enjoyed phenomenal success. However, in the past decade, it has become evident that the same periodontal disease processes that affect teeth affect dental implants.
Peri-implantitis is defined as an inflammatory process affecting the tissues around an osseointegrated implant that results in loss of the supporting alveolar bone. Clinically it is present when three conditions are seen: radiographic evidence of bone loss exceeding the typical anatomic remodeling, pocket depths greater than 5 mm, and bleeding or suppuration on probing ( Figure 25-1, A and B ). The precursor to peri-implantitis is termed peri-implant mucositis ( Figure 25-1, C ), which is basically peri-implantitis without concomitant bone loss and which may be reversible with proper treatment. It is estimated that after 5 years, nearly 50% of implant sites may develop peri-implant mucositis. Peri-implant mucositis typically is treated nonsurgically, with curettage, chlorhexidine mouth rinse, and antibiotics.

Procedures to salvage dental implants are evolving. A study by Roos-Jansaker et al. in 2006 revealed a 12% incidence of peri-implantitis after 10 years in a European population. Recent studies have confirmed the undeniable prevalence of this problem. In a review of the epidemiology of peri-implantitis, Mombelli et al. stated that the prevalence of peri-implantitis is on the order of 10% of implants and 20% of patients after 5 to 10 years. Most studies also conclude that smoking and a history of periodontitis significantly affect a patient’s predisposition to developing peri-implantitis.
Peri-implantitis results in the loss of supporting bone and soft tissue. Treatment may involve removal of the implant (deplantation), débridement procedures, and regenerative procedures in conjunction with débridement. In the 1990s and early in the 2000s, many of the studies on peri-implantitis were done in the canine model using ligature-induced peri-implantitis. However, over the past decade, enough implants have been placed in the general population to allow studies using implants in patients.
It has been shown that reosseointegration can occur on a repaired surface. Reintegration may consist of soft tissue reattachment, osseous reattachment, or a combination of the two. Protocols for regenerative procedures are evolving; they include the use of allogeneic bone graft materials, autogenous bone graft materials, and commercially available tissue engineering products, such as recombinant human bone morphogenic protein (rhBMP) and recombinant platelet-derived growth factor (rhPDGF). Success rates vary, depending on the anatomy and amount of preexisting bone loss, but typically are in the 60% to 70% range. When an ideal repair situation exists, success rates approach 100%. In 2012 Heitz-Mayfield et al. reported a 47% elimination of bleeding on probing and a 92% level of resolution of bone loss after 12 months of antiinfective treatment combined with open débridement.
The etiology of peri-implantitis is multifactorial. One of the most common causes is retained cement from cementation of a prosthesis. If inflammation develops within weeks or months after crown cementation, surgical exploration for retained cement is indicated ( Figure 25-2 ).

Another common cause is periodontally compromised teeth elsewhere in the mouth. Studies have shown that pocket depths of 6 mm or more around teeth cause the seeding of implants with periodontal pathogens; peri-implantitis presents itself with a lag time of approximately 2 to 3 years after pocket development. Considerable research is under way regarding a genetic component underlying the individual susceptibility to implant loss. The interleukin-1 and interleukin-6 genes have been studied and may offer an explanation for the clusterization phenomenon, in which certain individuals appear to be susceptible to chronic periodontitis and peri-implantitis, resulting in an increased incidence of implant loss.
Other common causative factors include a poor prosthesis design that inhibits hygiene, inadequate attached tissue, endodontic defects on adjacent teeth, and systemic issues, such as smoking and diabetes. These issues need to be addressed and eliminated, when possible, before the repair is undertaken.
It is interesting to note that when Brånemark and colleagues originally presented their 15-year success rates, their long-term success rates were high, and peri-implantitis was not a major problem in their patient population. This is likely due to the fact that the vast majority of their original patients were edentulous and had screw-retained prostheses. Their protocol thereby eliminated the two most common causes of peri-implantitis: retained cement and periodontal pathogens associated with periodontally compromised natural teeth.
Prevention of peri-implantitis starts with proper implant site development, obtaining optimized bone and soft tissue, and subsequent ideal implant placement. Prevention of periodontal disease elsewhere in the mouth, proper prosthesis design for adequate hygiene, prevention of retained cement, and regular hygiene recall for early detection of peri-implantitis are all necessary to minimize peri-implant disease.
Indications for the Use of the Procedure
Once the diagnosis of inflammation with bone loss has been made, the clinician must determine whether the implant is treatable. Unlike teeth, when implants are removed, they typically leave a sizable defect that does not have four walls. The resultant osseous regeneration often is minimal and typically requires aggressive bone grafting to regenerate the site for a new implant. For this reason, undergoing an implant salvage procedure is often in the patient’s best interest.
Typically, osseous defects of 5 to 6 mm or less vertically along the implant are amenable to treatment. Larger defects may be treated if the implants are critical in support of the prosthesis and removal may result in complete loss of a significant prosthesis. In the case illustrated in Figure 25-3 , implant #10 was vital to the prosthesis, and a repair was carried out, despite greater than 50% bone loss. The most treatable defects appear to be the circumferential crater type lesions caused by retained cement, which closely resemble a three- or four-wall periodontal defect ( Figure 25-4 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


