The old Boy Scout’s motto, “Be Prepared,” can be beneficially applied to the management of dental trauma. A large number of dental injuries occur every year, primarily in the 7- to 15-year age group. Preserving the natural dentition during that time period is critically important, because tooth loss at an early age presents significant lifelong dental problems. Being prepared to manage an emergency can make the difference between tooth loss and a successful outcome. Two factors contribute to achieving the better outcome: knowledge of the essentials of dental traumatology, and being prepared with the dental materials needed for appropriate treatment. It is the hope of the authors that these factors are clearly elucidated in this article.
Traumatic dental injuries tend to be unexpected and injured patients typically arrive in the dental office on an emergency basis. They have to be fitted in, often in a busy schedule, and not much time is available to examine, plan procedures, discuss options, and provide treatment. Yet, they need attention, and in some cases, the length of time between accident and treatment is critical for a successful outcome. Therefore, it makes sense that a dental office to which patients with dental injuries may come, would be prepared to provide efficient and correct emergency treatment.
To be well prepared for traumatic dental injuries, it helps to recognize that such injuries vary in terms of urgency for treatment. Andreasen and colleagues have recommended treatment priorities based on the effect of time between accident and treatment. The time frames indicated are for the purpose of predicting best outcomes. Teeth can be treated after the ideal time frame and still experience successful outcomes.
-
Treatment priorities
- 1.
Acute. Should be treated within a few hours. Injuries include: avulsions, extrusions, lateral luxations, and root fractures.
- 2.
Subacute. Should be treated within 24 hours. Injuries include: intrusions, subluxations, crown fractures with pulp exposure.
- 3.
Delayed. Can be delayed more than 24 hours. Injury: crown fractures without pulp exposure.
Classification and treatment priorities
The emphasis in this article will be dental traumatic injuries involving teeth and the periodontal ligament. Soft tissue injuries (ie, lacerations, contusions, and abrasions) are usually managed in emergency rooms and will not be included here.
Enamel Fractures
Enamel fractures only involve enamel and no urgency exists. Treatment can be performed at any time.
Uncomplicated Crown Fracture
Uncomplicated crown fractures involve enamel and dentin but not the pulp ( Fig. 1 ). There is low treatment priority (delayed); outcome is not affected if treatment is delayed more than 24 hours. The tooth should, however, be kept clean to prevent bacterial growth on the exposed dentin surface.

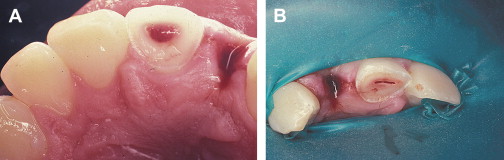
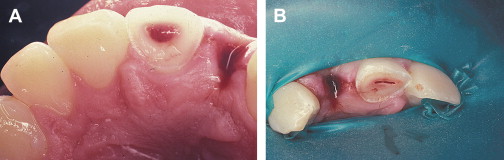
Complicated Crown Fracture
Complicated crown fractures involve enamel, dentin, and pulp ( Fig. 2 ). Priority is subacute, which means that treatment should be done as soon as possible, preferably within 24 hours. The pulp, however, can survive for many hours as long as it is healthy. This type of injury can be treated with a pulp cap or shallow pulpotomy. If the tooth is a fully formed tooth in an adult and root canal treatment is chosen, it can be done at a time convenient for the patient and the dentist.
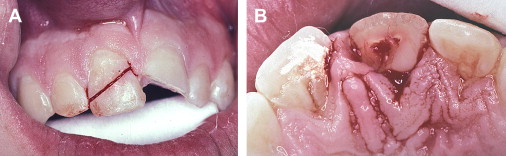
Crown-root Fracture
Crown-root fractures involve enamel, dentin, and cementum, and possibly the pulp ( Fig. 3 ). Treatment priority is similar to crown fractures, depending on whether or not the pulp is involved.
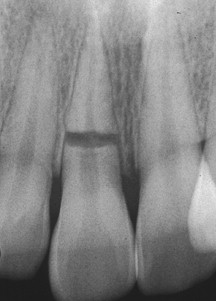
Root Fracture
Root fractures involve cementum, dentin, and pulp ( Fig. 4 ). They are usually horizontal or diagonal. Treatment priority is acute, particularly if the coronal segment has been displaced. Treatment consists of repositioning to coronal segment and stabilizing the tooth for 4 to 6 weeks. Variations in treatment may be dictated by the fracture position; fractures close to the crest of the alveolar bone may benefit from extended splinting periods.
Luxation Injuries
Luxation injuries involve the teeth and the periodontal ligament (PDL), and may also involve the supporting alveolar bone ( Fig. 5 ). The injuries can be identified into five categories: concussion, subluxation, extrusive luxation, lateral luxation, and intrusive luxation.

Concussion
Concussion involves the tooth and the PDL. The tooth is painful to percussion, but has not been displaced and healing is usually uneventful, particularly in young patients. No treatment is indicated other than symptomatic attention, such as avoiding biting hard on the tooth until it is comfortable. Monitoring the tooth for possible pulpal deterioration is indicated, particularly in mature, fully developed teeth.
Subluxation
Subluxation involves the tooth, the PDL, and also some minor damage to the supporting alveolar bone. Treatment priority is subacute. The tooth is painful to percussion and has increased mobility compared with adjacent uninjured teeth. No treatment is usually needed, but stabilization for a short period of time (ie, 2–4 weeks) will provide patient comfort. Subluxated teeth must be monitored for pulpal deterioration, particularly in mature, fully developed teeth.
Extrusive luxation
Extrusive luxation involves the tooth, the PDL, and possibly the supporting alveolar bone. The tooth will be mobile compared with uninjured adjacent teeth and will probably be sensitive to percussion; it will be partially extruded from the alveolar socket. Treatment consists of repositioning the tooth into its original location and stabilizing the tooth for 4 weeks. Treatment priority is acute. In immature, developing teeth with apical openings greater than 1 mm in diameter, pulpal revascularization is possible, but not predictable. In mature fully developed teeth, pulpal revascularization is not expected and root canal therapy is recommended. Endodontic treatment can be initiated 10 to 14 days after the initial emergency treatment of repositioning and splinting.
Lateral luxation
Lateral luxation involves the tooth, the PDL, and the supporting alveolar bone. The tooth has been displaced and often the apical part of the root has been forced into the adjacent bone making the tooth appear ankylosed, without mobility. It is usually not overly painful to percussion. Treatment priority is acute. Treatment consists of repositioning the tooth into its original position, stabilizing it for 4 weeks, during which time root canal treatment is recommended and can be initiated 10 to 14 days after emergency treatment if the tooth is fully developed. Young, immature teeth have the potential for pulpal revascularization, but it is not predictable.
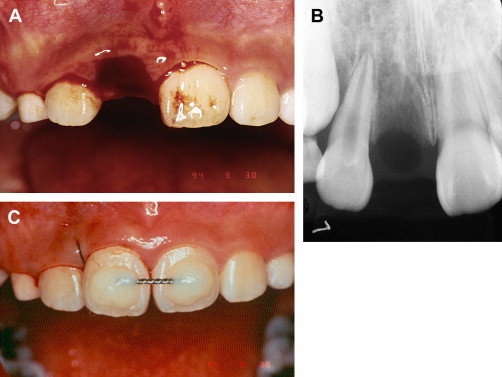
Intrusive luxation
Intrusive luxation involves the tooth, the PDL, and the supporting alveolar bone. The tooth is completely firm because it has been displaced vertically into the alveolar bone. It appears ankylosed and is usually not painful to percussion. Treatment priority is subacute, but it depends on the patient’s age. Children under the age of 15 have the potential for intruded teeth to spontaneously re-erupt. When that happens, the outcome of the traumatic injury leads to the best possible result. In patients over the age of 15, the intruded teeth should be repositioned either orthodontically or surgically, and root canal therapy is recommended. The endodontic treatment can be initiated within 10 to 14 days after repositioning the tooth surgically, or as soon as accessible if repositioned orthodontically. After repositioning, regardless of technique, the tooth needs to be stabilized for 4 weeks.
Avulsion
In avulsion, the tooth has been completely ex-articulated from its socket ( Fig. 6 ). Treatment priority is acute and consists of replanting the tooth in a most timely manner. Ideally, avulsed teeth should be replanted at the site of injury; the outcome is directly related to the time the tooth is away from its normal environment. If the patient, or the person helping the patient, is unable to replant the tooth on site, it can be transported with the patient, either in the patient’s mouth (saliva is an acceptable transport medium) or in a cup of milk which is also an excellent transport medium.
Following replantation, the tooth should be stabilized for at least 2 weeks during which the endodontic treatment can be initiated (ie, 10–14 days). The only exception to including root canal treatment in the management of an avulsed tooth is if it is an immature tooth with a wide open apex, in which revascularization is desirable and may occur. Close monitoring is essential, because infection-related inflammatory root resorption can be very aggressive if it takes place, particularly in young teeth.
Classification and treatment priorities
The emphasis in this article will be dental traumatic injuries involving teeth and the periodontal ligament. Soft tissue injuries (ie, lacerations, contusions, and abrasions) are usually managed in emergency rooms and will not be included here.
Enamel Fractures
Enamel fractures only involve enamel and no urgency exists. Treatment can be performed at any time.
Uncomplicated Crown Fracture
Uncomplicated crown fractures involve enamel and dentin but not the pulp ( Fig. 1 ). There is low treatment priority (delayed); outcome is not affected if treatment is delayed more than 24 hours. The tooth should, however, be kept clean to prevent bacterial growth on the exposed dentin surface.

Complicated Crown Fracture
Complicated crown fractures involve enamel, dentin, and pulp ( Fig. 2 ). Priority is subacute, which means that treatment should be done as soon as possible, preferably within 24 hours. The pulp, however, can survive for many hours as long as it is healthy. This type of injury can be treated with a pulp cap or shallow pulpotomy. If the tooth is a fully formed tooth in an adult and root canal treatment is chosen, it can be done at a time convenient for the patient and the dentist.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


