The literature on the anatomy and physiology of the paranasal sinuses goes back to Galen (AD 130-201), who referred to the “porosity” of the bones of the head. Leonardo da Vinci (1452-1519), whose classical sections of the head illustrate the maxillary antrum and the frontal sinus, apparently recognized the existence of these cavities as separate functional entities. He also referred to the maxillary sinus as “the cavity of the bone which supports the cheek.” In 1651 Highmore was the first to give a detailed description of the maxillary antrum (antrum of Highmore). However, it was only in the late nineteenth century that the first detailed and systematic anatomic and pathologic descriptions of the paranasal sinuses were published by Zuckerkandl. These descriptions became even more valuable because they could be applied directly to patients and their problems.
The invention of the x-ray technique did not add much to the anatomic knowledge of the sinuses. However, computed tomography (CT), available since the mid-1970s, made the relationship between the largest sinuses and the ethmoids very clear, applying the knowledge that had been developed more than 100 years earlier. Comparisons of CT images with the drawings of Onodi, Grunwald, and Zuckerkandl demonstrate the incredible accuracy of these pioneers’ knowledge.
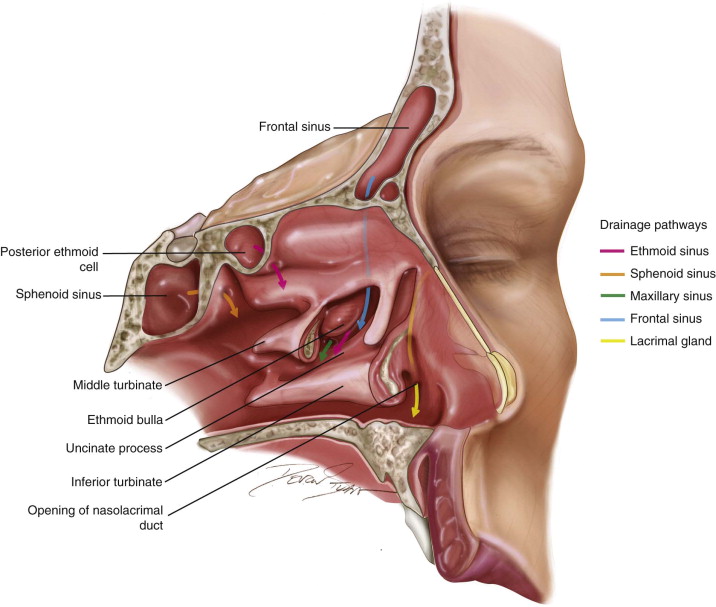
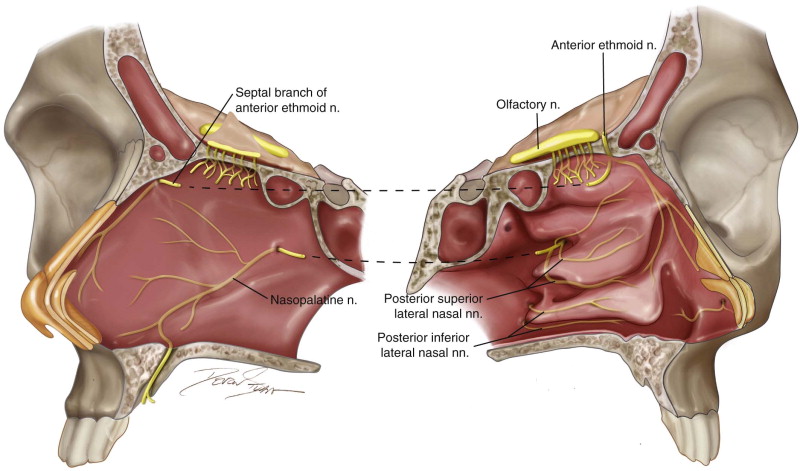
The paranasal sinuses form a complex unit of four paired air-filled cavities at the entrance of the upper airway: the ethmoidal, sphenoidal, maxillary, and frontal sinuses ( Figure 3-1 ). Each of the sinuses is named according to the bone in which it is found. The paranasal sinuses develop as outgrowths from the nasal cavities and erode into the surrounding bones. All these cavities are lined by respiratory mucosa, which is ciliated and secretes mucus. All the paranasal sinuses open into the nasal cavity ( Figure 3-2 ). These sinuses are innervated by the branches of the trigeminal nerve ( Figure 3-3 ).
The paranasal sinuses start developing from ridges and furrows in the lateral nasal wall as early as the eighth week of embryogenesis, and they continue pneumatization until early adulthood. As mentioned, each one is named after the skull bone in which it is located. However, during the development of a sinus, pneumatization may involve adjacent bones; for example, the ethmoid sinus develops into the frontal, maxillary, or sphenoid bone, and the maxillary sinus extends into the zygomatic bone.
All sinuses are lined by a respiratory pseudostratified epithelium composed of four major types of cells:
- •
Ciliated columnar cells
- •
Nonciliated columnar cells
- •
Goblet-type mucous cells
- •
Basal cells
This mucosa is directly attached to bone and is referred to as the mucoperiosteum. Although it is somewhat thinner, the mucoperiosteum of the sinuses is continuous with that of the nasal cavity through the various ostia of the sinuses. The ostium is a natural opening through which the sinus cavity drains into the airway, either directly into the nasal cavity (sphenoid ostium) or indirectly by means of more complex anatomic structures (frontal recess).
Ethmoidal Sinus
The ethmoid sinus begins forming in the third to fourth month of fetal life as evaginations of the lateral nasal wall. At birth the anterior ethmoid cells are aerated, whereas the posterior ethmoid cells are fluid filled. The posterior ethmoid air cells pneumatize with advancing age, and air replaces the fluid in these cells. The last air cells to finish forming are the anterior-most agger nasi and bulla cells. When pneumatization is complete, the average size of the anterior ethmoid cells is 20-24 × 20-24 × 10-12 mm, and the average size of the posterior ethmoid cells is 20-21 × 20-22 × 10-12 mm.
Ethmoid Air Cells
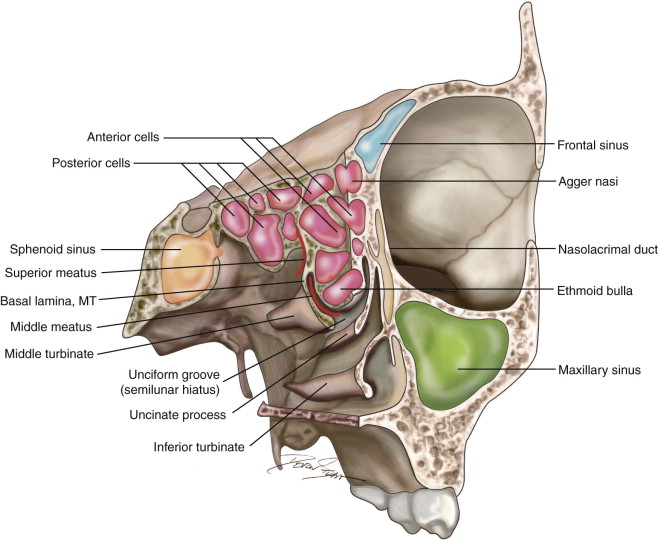
Within the labyrinth lie the ethmoid air cells, which are lined by pseudostratified ciliated columnar epithelium. The ethmoid air cells are bordered medially by the nasal cavity, laterally by the lamina papyracea, and superiorly by the fovea ethmoidalis. The basal lamina of the middle turbinate divides he ethmoid cells into anterior and posterior divisions. The anterior cells empty into the middle meatus, and the posterior cells drain into the superior meatus.
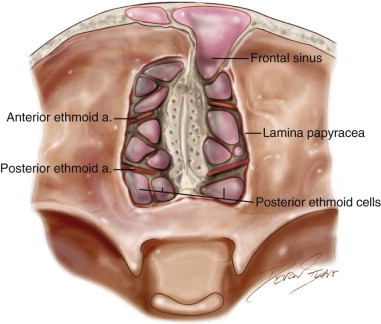
Hajek presented a simplified scheme to describe the location of the ethmoid air cells. Hajek’s scheme depicted the air cells as existing in three sets of grooves, which form as valleys between four lamellar projections of bone. Anteriorly the unciform groove (hiatus semilunaris) is formed by the unciform process anteriorly and the ethmoid bulla posteriorly; the hiatus semilunaris is the site of orifices to the frontal sinus, maxillary sinus, and anterior ethmoidal cells. The second groove is the middle meatus, which lies between the ethmoid bulla anteriorly and the middle turbinate posteriorly; the ethmoid bulla located in this lamella is often involved in nasofrontal duct obstruction. The third groove is the superior meatus that is formed between the middle and superior turbinates ( Figure 3-4 ). The numbers of ethmoid cells vary by individual; however, seven smaller anterior cells and four larger posterior cells are typically present. The posterior air cells occasionally present as two very large air cells. The uncinate groove is the most anterior and has three to four air cells at its superior border. At the middle meatus are one to two agger nasi cells, and posterior to the agger nasi is the ethmoid bulla that contains a superior and inferior cell. The posterior ethmoid air cells drain via the superior meatus. The anterior ethmoid air cells drain via the middle meatus. Arterial supply to the ethmoid air cells is via the ethmoidal arteries that are branches from the ophthalmic artery. The anterior ethmoidal artery enters the anterior ethmoid foramen 24 mm posterior to the anterior lacrimal crest and supplies the anterior ethmoid air cells. The posterior ethmoidal artery enters the posterior ethmoid foramen 36 mm posterior to the anterior lacrimal crest and supplies the posterior ethmoidal air cells. Venous drainage is via the named veins accompanying the arteries to the superior ophthalmic vein or pterygopalatine plexus. Lymphatic drainage from the anterior ethmoid cells is via the submandibular nodes, and the posterior ethmoid cells drain via the retropharyngeal nodes. Innervation is via anterior and posterior ethmoid nerves of the ophthalmic nerve (V1) and the posterior nasal branch of the maxillary nerve (V2).
Maxillary Sinus
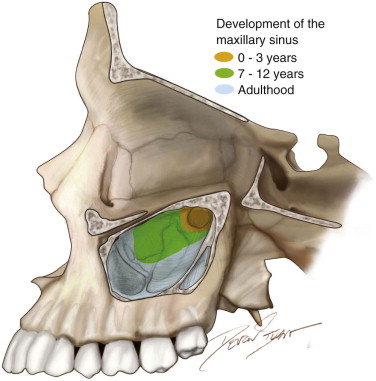
The maxillary sinus begins developing in the third week of gestation. In the twelfth week of gestation, the maxillary sinus forms as an ectodermal invagination from the middle meatal groove and grows internally to a size that at birth is approximately 7 × 4 × 4 mm and has a volume of 6 to 8 mL. In utero the maxillary sinus is fluid filled; however, after birth the maxillary sinus pneumatizes in relation with biphasic rapid growth: during the first 3 years of life and then again from ages 7 to 12 years. By 12 years of age, the sinus is level with the floor of the nasal cavity ; however, as further pneumatization occurs into adulthood, with the eruption of the adult molars, the floor of the sinus descends to approximately 1 cm below the floor of the nasal cavity.
The maxillary sinuses are paired paranasal sinuses that develop around the adult dentition to a volume of 15 mL, although the volume is smaller in children and enlarges with the sinus pneumatization that occurs with advancing age. The span of these sinuses is from the region of the third molar posteriorly to the premolar teeth anteriorly. The dimensions of the sinus vary and range from 25 to 35 mm mesiodistal width, 36 to 45 mm vertical height, and 38 to 45 mm deep anteroposteriorly. Mesiodistal width differences are usually attributed to growth toward the zygomatic arch posteriorly rather than toward the canine teeth anteriorly.
The maxillary sinus is shaped like a quadrangular pyramid, with the base facing the lateral nasal wall and the apex oriented at the zygomatic arch. The roof of the sinus contributes to the floor of the orbit, the floor faces the alveolar process, and the sinus proceeds deep and adjacent to the palate. The schneiderian membrane lines the maxillary sinus and is composed of pseudostratified ciliated columnar epithelium. The concentration of cilia increases with proximity to the sinus ostium. The thickness of this membrane is 0.8 mm. Compared with the nasal mucosa, the antral mucosa is thinner and less vascular. At birth, the maxillary sinus begins medial to the orbit, and its dimensions are largest anteroposteriorly. At 2 years of age, the sinus continues inferiorly below the medial orbit and continues to pneumatize laterally. By 4 years of age, the sinus reaches the infraorbital canal and continues laterally. By 9 years of age, inferior growth reaches the region of the hard palate. Pneumatization continues as the permanent teeth erupt.
The roof of the maxillary sinus contributes to the floor of the orbit. The roof contains the infraorbital neurovascular bundle. The infraorbital foramen opens approximately 1 cm below the infraorbital rim. The floor of the maxillary sinus abuts the alveolar process of the maxilla, frequently approximating the apices of the molar teeth (see the next section). The inferior extent of the sinus floor is 1 cm inferior to the floor of the nasal cavity. The medial wall of the maxillary sinus houses the sinus ostium at its superomedial aspect and the nasolacrimal duct, through which drainage of the lacrimal apparatus occurs. The maxillary sinus ostium empties into the posterior aspect of the semilunar hiatus. The nasolacrimal duct runs 4 to 9 mm anterior to the sinus ostium and empties at the anterior portion of the inferior meatus.
Sinus development follows a three-compartment model described by Underwood in which these compartments, frequently separated by septa, are associated with three different dental milestones. The anterior compartment forms around the primary molars between 8 months and 2 years of age. The middle compartment forms around the adult first and second molars from 5 to 12 years of age. The posterior compartment forms around the third molars from 16 to 30 years of age. The most inferior portion of the maxillary sinus is in the region of the first molar. The distance from the sinus floor to the root tips of the teeth is longest for the first premolar and shortest for the second molar distobuccal root tip. The roots of the maxillary first and second molars communicate with the floor of the maxillary sinus with an incidence of 40%. The palatine roots of these teeth are 50% closer to the antral floor than to the palate, and in 20% of cases apical communication is present between the palatal roots of the maxillary first and second molars with the maxillary sinus ( Figure 3-5 and Table 3-1 ).
| Root | Distance (mm) | SD |
|---|---|---|
| Buccal first premolar | 6.18 | 1.60 |
| Lingual first premolar | 7.05 | 1.92 |
| Second premolar | 2.86 | 0.60 |
| Mesiobuccal first molar | 2.82 | 0.59 |
| Palatal first molar | 1.56 | 0.77 |
| Distobuccal first molar | 2.79 | 1.13 |
| Mesiobuccal second molar | 0.83 | 0.49 |
| Palatal second molar | 2.04 | 1.19 |
| Distobuccal second molar | 1.97 | 1.21 |
Maxillary Septum
A septum is defined as a strut of bone that is at least 2.5 mm in height. Septa within the maxillary sinus are of two varieties. The primary septa are formed as part of the three-compartment model of sinus development and act as dividers of the anterior, middle, and posterior components; they are found between the roots of the second premolar and the first molar and the roots of the first and second molars, and distal to the roots of the third molar. Septa extrinsic to those of maxillary development are called secondary septa and occur as a result of pneumatization after dental extraction. The overall prevalence of septa present in any given maxillary sinus is 35%. Septa in edentulous regions tend to be larger than those in partially edentulous regions, which are larger still than dentate regions of the alveolus. The presence of septae is pertinent for sinus lift procedures because they complicate the process of luxating the bony window to expose the sinus and increase the likelihood of sinus membrane perforation.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


