The Neurocranium
The oft-heard maxim “anatomy is destiny” was coined by Sigmund Freud in summary of his assertion that gender is the primary determinant of personality traits. For surgeons, the same quote may be applied to the importance of mastering the intricate construction of the portion of the human body for which they are responsible. Thorough comprehension of anatomy allows the surgeon to work safely and precisely, thereby optimizing restoration of health and minimizing morbidity. In this chapter, the structure of the neurocranium and how it relates to oral and maxillofacial surgery are examined.
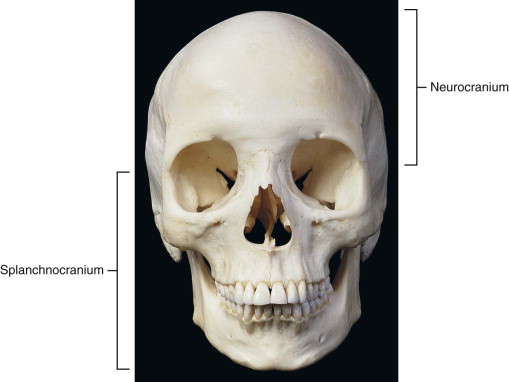
The skull consists of the cranium ( Figure 1-1 ) and the mandible ( Figure 1-2 ). The cranium is divisible into the neurocranium and the splanchnocranium (see Figure 1-1 ). The neurocranium encases the brain and is found above the orbits. Below the orbits, the viscerocranium, alternately called the splanchnocranium or midface, supports the nasal passages and the oral cavity and makes up the face.

The neurocranium may be considered in two parts: the roof, or cranial vault (also called by its Latin name, the calvaria ), and the floor, or cranial base. The space within the neurocranium occupied by the brain is the cranial cavity. The calvaria is formed anteriorly by the frontal bone, posteriorly by part of the occipital bone, and laterally by the paired parietal bones and squamous portions of the temporal bones ( Figure 1-3 ). Although most bones develop by endochondral ossification, which involves formation of a cartilaginous template that is gradually replaced by bone, the bones of the calvaria develop through intramembranous ossification, whereby mesenchymal cells forming a membrane over the brain condense into a collection of nodes and differentiate directly into osteoblasts. The osteoblasts secrete a matrix that becomes calcified, resulting in the formation of flattened bone within the membrane. The nodes or islands of bone enlarge radially, but at birth the bones of the calvaria are still separated from each other by the mesenchymal membrane. The largest areas of noncalcified membrane, which are called fontanelles , are found where the frontal and occipital bones meet the parietal bones on the superior aspect of the calvaria (see Figure 1-3 ). The failure of the calvarial bones to fuse prior to infancy allows the cranium to deform during passage through the birth canal and also allows the volume of the neurocranium to continue to expand after birth to accommodate enlargement of the brain. Intramembranous ossification continues through infancy until the bones of the calvaria meet and form fibrous suture joints, which usually fuse during adulthood.
One or more of the sutures between the bones of the calvaria may prematurely fuse during fetal development. Virchow’s Law states that this event, which is called craniosynostosis, results in imbalanced development of the skull; enlargement perpendicular to the fused suture is limited, and enlargement of the area where the sutures remain open is correspondingly increased. The resulting malformation has the potential to cause compression of a portion of the brain, which may result in neurologic abnormalities.
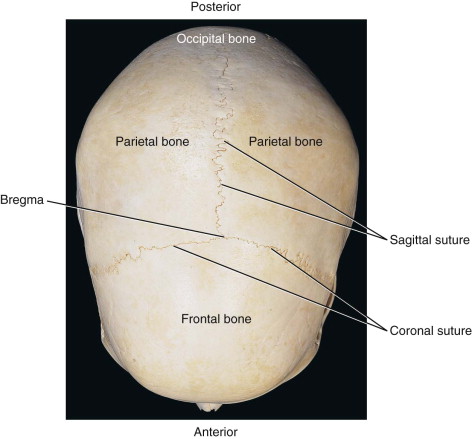
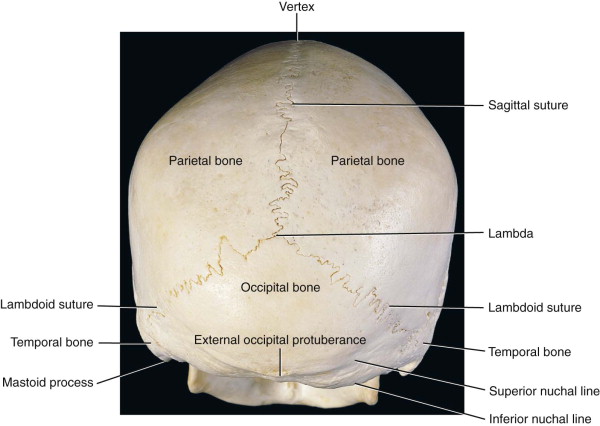
After fusion, the sutures remain visible on the external and internal surfaces of the calvaria (see Figure 1-3 ). Along the midline, the sagittal suture is located between the left and right parietal bones. The vertex, a conceptual point indicating the apex of the skull, would be located on the sagittal suture on a perfect skull. On the internal surface of the calvaria, an indentation is normally visible along the midline that corresponds to the superior sagittal sinus, a venous sinus within the dura mater (this is discussed in more detail with the cranial base). The coronal suture runs between the frontal bone and parietal bones, and the lambdoid suture is found between the occipital bone and the parietal bones. The sagittal suture intersects the coronal suture at the bregma and the lambdoid suture at the lambda ( Figure 1-4 ).
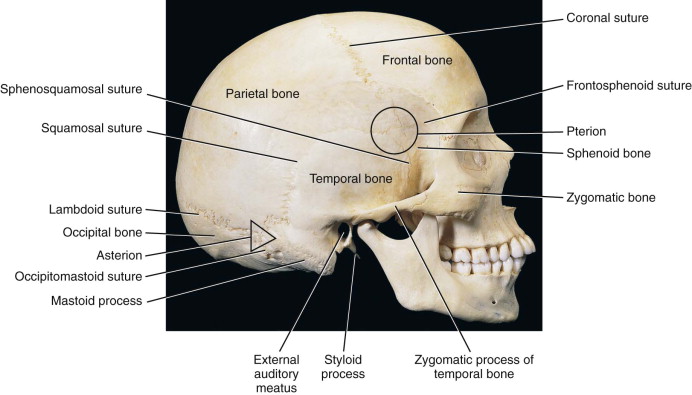
Bilaterally on the calvaria, the squamosal suture is visible between the parietal bone and the squamous portion of the temporal bone. The area where the parietal, temporal, and occipital bones meet is called the asterion, which serves as a neurosurgical landmark. More anteriorly, the frontal, parietal, and temporal bones intersect with a bone involved in the formation of the cranial base, the sphenoid bone, to form an H -shaped suture called the pterion ( Figure 1-5 ). The middle meningeal artery, which arises from a branch of the external carotid artery called the maxillary artery, runs along the inside of the neurocranium and crosses the pterion. Trauma to the skull at the pterion can rupture the underlying middle meningeal artery, leading to a potentially fatal epidural hematoma.
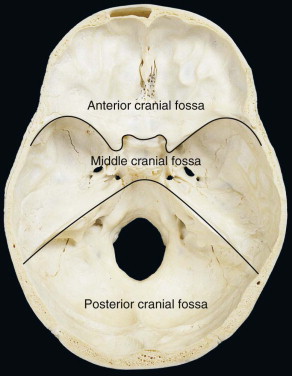
The floor of the neurocranium is formed by the occipital, temporal, sphenoid, ethmoid, and frontal bones. The internal surface of the floor of the neurocranium, upon which the brain rests, may be divided into the anterior, middle, and posterior cranial fossae ( Figure 1-6 ).
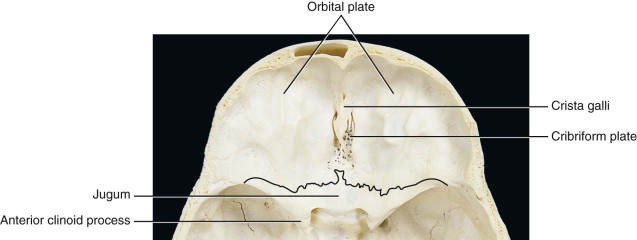
The majority of the anterior cranial fossa consists of the orbital plates of the frontal bone, which form the roofs of the orbits. The orbital roofs bear impressions that mirror the undulating sulci and gyri of the overlying cerebrum. An explanation of how the gelatinous brain might influence the structure of rigid bone is found in Melvin Moss’s functional matrix hypothesis, which states that development of bone sequentially follows, and is thus dependent on, structural changes in collections of developing soft tissues called functional matrices. The cerebrum would thus be a component of the functional matrix for which the associated bone is the frontal bone, or more specifically, the orbital plates of the frontal bone. Likewise, the superior sagittal sinus is a component of the functional matrix associated with the parietal bones; hence, the impression along the internal surface of the sagittal suture described earlier.
Part of the ethmoid bone is found between the orbital plates of the frontal bone ( Figure 1-7 ). The vertical ridge at the midline is the crista galli, named for its resemblance to a rooster’s crest. The cerebral falx, a vertical sheet of dura mater separating the cerebral hemispheres, attaches to the crista galli. On either side of the crista galli are the cribriform plates, which have numerous perforations. Branches of the first cranial nerve, the olfactory nerve, pass through these perforations to reach the nasal cavity.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


