Given the intimate association of the external auditory canal and middle ear space with the temporomandibular joint, it is necessary for oral and maxillofacial surgeons (OMS) to understand the auditory system. Disorders of the temporomandibular joint may sometimes present with primarily aural symptoms such as otalgia or aural fullness. This chapter describes the anatomy of the auditory system with an emphasis on information of interest to the OMS.
The peripheral components of the auditory system are housed within or attached to the temporal bone. The auditory system can generally be broken down into several smaller components, including the external ear, the middle ear and mastoid, the inner ear, and the central auditory system. Also important is the course of the facial nerve within the fallopian canal of the temporal bone. The OMS will also be interested in the adjacent sphenoid bone, the mandibular nerve as it enters the skull base at the foramen ovale, and the middle meningeal artery coursing through the foramen spinosum.
Temporal Bone
The temporal bones, which compose a portion of the lateral skull and skull base, have several components: the squamosa, petrous, mastoid, and tympanic portions, as well as the styloid process. These will be discussed briefly, with a focus on landmarks identified during surgical procedures.
The squamosa ( Figure 4-1 ) is the lateral, parasagittally oriented, flat bone that composes a portion of the lateral skull. The temporalis muscle attaches on its lateral surface, and the middle meningeal artery runs in a groove on its medial surface. On the anterior, inferior surface of the lateral squama, the zygomatic process extends laterally and anteriorly to make up the posterior portion of the zygomatic arch. The zygomatic process is contiguous with a horizontally oriented structure known as the suprameatal crest or temporal line, which runs superior to the external auditory canal. The temporal line is a surgical landmark roughly approximating the level of the floor of the middle cranial fossa. The squamosa forms the superior and anterior aspects of the mandibular or glenoid fossa of the temporomandibular joint. The inferior articular tubercle forms the superior boundary of the mandibular fossa and is lined with a thin layer of cartilage.
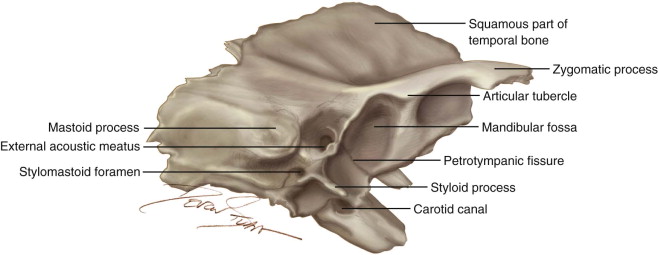
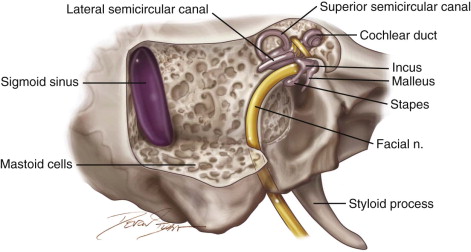
The mastoid comprises the posterior temporal bone and is the site of attachment of the sternocleidomastoid, splenius capitis, longissimus capitis, and digastric muscles. The mastoid process is typically aerated with numerous bony air cells. These air cells communicate anteriorly with the mastoid antrum. A groove in the medial mastoid houses the dural sigmoid sinus. The superior border of the mastoid is the bony plate that separates the mastoid from the middle cranial fossa, known as the tegmen mastoideum. During a mastoidectomy ( Figure 4-2 ), the bone overlying the sigmoid sinus and the tegmen are used as landmarks to indicate the posterior and superior limits of dissection. Medially, dissection can be continued until the lateral semicircular canal is visualized through the mastoid antrum.
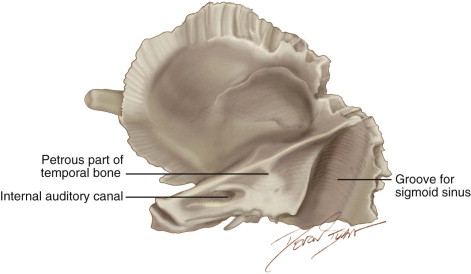
The petrous portion is a pyramidal-shaped bone with its apex pointing medially toward the clivus. During procedures within the middle cranial fossa, working on the superior surface, important structures can be identified as surgical landmarks. The arcuate eminence indicates the position of the underlying superior semicircular canal. Medial and anterior to the superior canal is the facial hiatus, where the greater superficial petrosal nerve exits the temporal bone to travel on the superior surface of the petrous bone. The posterior, medial ( Figure 4-3 ) surface of the petrous portion of the temporal bone forms the anterior boundary of the posterior cranial fossa. The internal auditory canal is located in this region and contains the seventh and eight cranial nerves as they travel laterally. The complicated inferior surface of the petrous bone (see Figure 4-1 ) includes the carotid canal and jugular bulb. The petrous apex is the most medial portion of the petrous bone, lying medial to the labyrinth. It is pneumatized in a minority of patients and otherwise composed of bone and marrow.
The styloid process is an elongated, narrow bony process arising from the undersurface of the temporal bone and extending inferiorly. It emanates just anterior to the stylomastoid foramen, where the facial nerve exits the fallopian canal.
The tympanic bone composes the bone of the external auditory canal, the structure of which is discussed in more detail later in the chapter. The anterior tympanic bone forms the posterior boundary of the glenoid fossa.
External Ear
Auricle
The auricle, or pinna, is the visible portion of the auditory system, made up of a cartilaginous framework. This complex, three-dimensional structure collects sound energy and directs it to the conducting system of the middle ear.
The auricle begins to form during the sixth week of development, derived from the first and second branchial arch. Condensations of mesoderm form the six hillocks of His, which develop into identifiable portions of the auricle. The first through third hillocks form the tragus, crus helicis, and helix; the fourth through sixth form the antihelix, antitragus, and lobule.
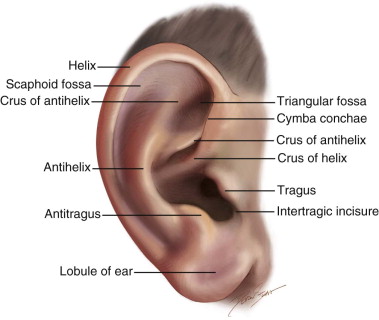
The adult auricle ( Figure 4-4 ) has a vertical height of 5 to 6 cm, and the helix sits 15 to 20 mm from the skin overlying the mastoid process. The helix comprises the smooth superior and posterior margin of the auricle and terminates anteriorly in the crus helicis or root of the helix. The crus helicis divides the conchal bowl into the superiorly located concha cymba and the more inferiorly located concha cavum. The antihelix is a vertically oriented structure that separates the helix from the conchal bowl. Superiorly, the antihelix divides to form the superior and inferior crura. The depression found between the superior and inferior crura is known as the fossa triangularis. The tragus is a triangular structure anterior to the meatus of the external auditory canal. Positioned opposite the conchal bowl, posterior and inferior to the tragus, sits the antitragus. The lobule is the inferior-most portion of the auricle and is devoid of cartilage.
A number of rudimentary muscles attach to the auricle, which are of little clinical significance in humans. The extrinsic muscles reposition the auricle in relationship to the head and include the anterior and posterior auricular muscles. The posterior auricular muscles are routinely encountered while making a postauricular incision, and their disruption leads to no significant clinical deficit. The intrinsic muscles include the transverse, oblique auricular, tragal, antitragal, as well as minor and major helical muscles.
Arterial supply to the auricle is via branches from the external carotid system and includes contributions from the superficial temporal, posterior auricular, and occipital arteries. The venous drainage corresponds with the feeding arterial supply.
Sensory innervation of the auricle involves multiple cranial and cervical nerves. Sensation is provided by the auriculotemporal nerve (CN V), sensory components of the facial nerve, Arnold nerve (CN X), and the greater auricular nerve (C2, 3).
The auricle is a valuable source of cartilaginous grafting materials for procedures in which semirigid grafting material is desired. A large, flat graft can be harvested from the tragus without cosmetic deformity if the lateral tragal framework is preserved. The entirety of the concha cavum and cymba can be harvested if the crus helicis, antihelix, and antitragus are preserved to maintain the structural framework of the auricle.
External Auditory Canal
The external auditory canal ( Figure 4-5 ) is a structure made up of an osseous and cartilaginous portion, extending from the conchal bowl to the tympanic membrane. From the concha, the external auditory canal is 2.5 cm in length, one third of which is cartilaginous and two thirds of which is osseous. The medial external auditory canal forms a groove known as the tympanic notch, which houses the tympanic annulus of the tympanic membrane. The anterior wall of the osseous canal makes up the posterior wall of the glenoid fossa of the temporomandibular joint.
The external auditory canal begins to form during the ninth week of embryogenesis and arises from the first branchial groove. The meatal plate, a solid core of ectoderm, extends toward the tympanic cavity. An intervening layer of mesoderm between the meatal plate and tympanic cavity persists at the fibrous layer of the tympanic membrane. The tympanic ring is ossified by the 15th week, leaving a superior defect in the ring known as the notch of Rivinus. Canalization of the ectoderm of the meatal plate begins at 21 weeks with canalization of the external auditory canal, a process that terminates at the 28th week of gestation. Developmental defects in this process can lead to canal stenosis or atresia.
The external auditory canal reaches adult morphology at approximately 9 years of age. The neonatal external auditory canal is a short and relatively straight structure with a nearly horizontal positioned tympanic membrane. During growth, the canal lengthens, becomes more tortuous for protection of the tympanic membrane, and the tympanic membrane assumes an oblique, anteromedial orientation with the posterior tympanic membrane situated lateral to the anterior portion. The skin overlying the lateral, cartilaginous canal is thicker than the skin of the osseous canal. This thicker skin contains the adnexal structures such as hair, sebaceous glands, and modified apocrine sweat glands, sometimes known as ceruminous glands. The transition from hair-bearing to non-hair-bearing skin within the external auditory canal is a good surgical landmark for the transition from the cartilaginous to osseous canal. The skin of the osseous canal is thin and firmly adherent to the bone of the canal. Two suture lines are readily identified during surgery involving the external auditory canal. The tympanosquamous suture is located along the anterosuperior canal, and the tympanomastoid suture is located posteroinferiorly. The skin is more firmly attached at these sutures and can be difficult to elevate due to fibrous attachments.
Two commonly described natural dehiscences of the external auditory canal allow infection or neoplasm to spread from within the canal. The fissures of Santorini are defects of the cartilaginous canal due to natural cleavage planes within the cartilage of the anterior canal. This dehiscence allows neoplastic and infectious processes to spread to the anteriorly located parotid gland. The foramen of Huschke is an anteriorly located dehiscence formed due to incomplete ossification of the tympanic ring. This can likewise facilitate the spread of neoplasm or infection, but it has also been a source of spontaneous sialorrhea. Furthermore, this defect of bone can allow for inadvertent entry into the external auditory canal, tympanic membrane perforation, and even ossicular injury during temporomandibular joint arthroscopy.
Multiple cranial nerves provide sensory innervation of the external auditory canal, which can explain pain referred to the ear canal. The auriculotemporal branch of the mandibular nerve innervates the anterior aspect of the canal, whereas the auricular branch of the vagus nerve innervates the posterior canal. Branches of the facial and glossopharyngeal nerves also mediate sensory input. The contribution of the facial nerve, which also innervates a portion of the auricular concha, explains the vesicular eruption seen with facial paralysis due to viral reactivation in Ramsay Hunt syndrome.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


