Armamentarium
|
History of the Procedure
The orbital box osteotomies are used to correct vertical or horizontal malposition of the entire orbit and its contents. The orbital box osteotomy was first performed by Paul Tessier to correct hypertelorism. He described osteotomies that separate the entire bony orbit from the skull and surrounding facial bones by combining both intracranial and facial approaches. Converse and Smith described subcranial U -shaped orbital osteotomies to correct hypertelorism; however, these techniques produced limited results. Schmid described circumferential orbital osteotomies to mobilize and translocate the orbits medially by an extracranial approach in patients with pneumatized frontal sinuses.
History of the Procedure
The orbital box osteotomies are used to correct vertical or horizontal malposition of the entire orbit and its contents. The orbital box osteotomy was first performed by Paul Tessier to correct hypertelorism. He described osteotomies that separate the entire bony orbit from the skull and surrounding facial bones by combining both intracranial and facial approaches. Converse and Smith described subcranial U -shaped orbital osteotomies to correct hypertelorism; however, these techniques produced limited results. Schmid described circumferential orbital osteotomies to mobilize and translocate the orbits medially by an extracranial approach in patients with pneumatized frontal sinuses.
Indications for the Use of the Procedure
The orbital box osteotomy is used to correct malpositions of the zygoma, orbit, and its contents in all planes. It is primarily indicated to correct hypertelorism. However, the box osteotomy can be used to correct vertical or horizontal dystopia due to congenital, pathologic, or traumatic abnormalities.
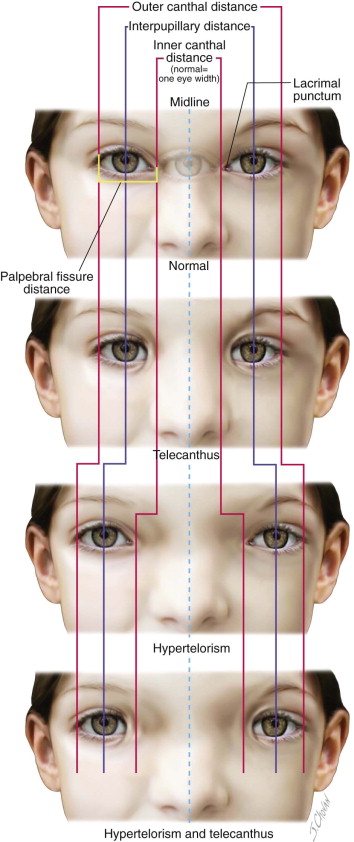
Orbital hypertelorism is an abnormally increased distance between the orbits. In this condition, the distance between the medial canthi, medial, and lateral walls of the orbit and the pupils is greater than normal. This is different from telecanthus, where the distance between the medial canthi is greater than normal and the distance between lateral walls of the orbit and pupils is normal ( Figure 47-1 ).
Orbital hypertelorism is an anatomic condition associated with a heterogeneous group of congenital disorders. This can occur as an isolated sporadic anomaly or with conditions such as Edwards syndrome (trisomy 18), basal cell nevus syndrome, craniofrontonasal dysplasia, DiGeorge syndrome, Apert syndrome, and Crouzon syndrome. A heterogeneous collection of frontonasal malformations is the group that most commonly displays hypertelorism ( Figure 47-2 ). The clinical findings in this group are usually symmetric hypertelorism, exaggerated widow’s peak onto the forehead, abnormal and wide-set eyebrows, down-slanting eyes, epicanthic folds, amblyopia, strabismus, a wide nose with a short philtrum, increased intrazygomatic distance, lateral and inferior positioned zygomas, median cleft lip, and a high arched palate. Other congenital conditions associated with hypertelorism are frontal encephaloceles, craniofacial clefts, and craniofrontonasal dysplasia ( Figure 47-3 ).



The other pathologic process for orbital dystopia is a slow-growing tumor such as neurofibromatosis, frontal sinus mucocele, and the like. Also, some of the high-energy injuries or inadequate corrections can cause orbital dystopia in vertical or horizontal positions ( Figure 47-4 ).

The surgery to correct hypertelorism is usually done when the patient is between 5 and 8 years of age. This timing addresses the psychosocial aspects of the developing child in the early school years. The physiologic reasons include the fact that the majority of the interzygomatic width is established by 6 years of age and there is adequate descent of tooth buds into the maxilla, giving space to make an osteotomy below the infraorbital nerve. The disadvantages are that the orbital bones before 5 years of age are thin and fragile and most patients who undergo correction of hypertelorism before the age of 8 by orbital osteotomies may require additional procedures for nasal correction in the future. The best and most stable results for hypertelorism correction are in the adult or nongrowing patient. This could be because the orbital bones are thicker and allow for more stable skeletal fixation.
The correction of orbital hypertelorism by box osteotomies should include correction of the nasal deformities. Bone and cartilage grafts may be necessary to create a nasal frame. Skin grafts may also be required for nasal coverage and can be accomplished with the use of local rotation flaps (i.e., forehead flaps) or advancement flaps. In the presence of meningoceles, it is important to bone-graft the cranial base defect to minimize recurrence of the lesion.
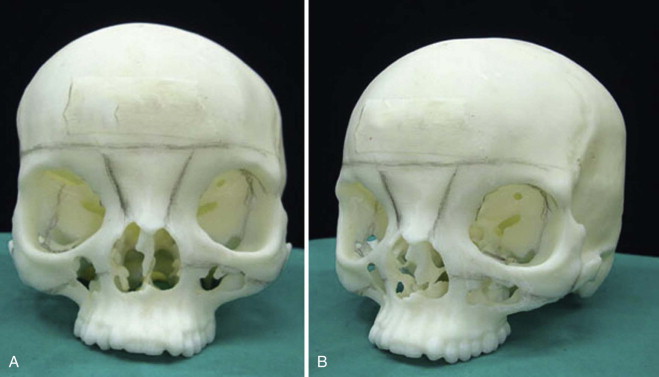
The preoperative planning for orbital box osteotomies should include evaluation by ophthalmology and neurosurgery specialists. These patients may have amblyopia, extraocular muscle dysfunction, or possibly develop binocular diplopia postsurgery. The surgical planning should include high-quality computed tomography (CT) scans with three-dimensional reconstructions. Stereolithographic models are also valuable for visualizing, marking, teaching, and understanding the osteotomies ( Figure 47-5 ).
Limitations and Contraindications
No specific contraindication exists for the procedure. However, medical issues may mitigate the performance of this procedure due to significantly increased morbidity, especially in the patient with considerable congenital heart disease. One noteworthy limitation of the procedure is that the correction only occurs in the orbital region. Only the orbital width is corrected (narrowed). In patients who also have slanting of the facial halves or who require expansion of the transmaxillary width, a facial bipartition procedure is more ideally suited for correcting the entire facial deformity.
Technique: Orbital Box Osteotomy
Step 1:
Patient Positioning, Airway and Corneal Protection
An oral RAE tube is used and secured to the midline by tape or to the lower two central incisor teeth using a 24-gauge wire. The upper and lower eyelids are sutured closed by a single horizontal mattress suture after placement of ophthalmic ointment to protect the cornea.
The coronal incision is marked, using a zigzag pattern, especially at the temporal region. A small 1-cm strip of hair is trimmed along the planned coronal incision.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


