Fig. 5.1
Dry mouth and dietary intake. The figure illustrates by arrows possible interactions between dry mouth and dietary intake
Although, theoretically several conditions related to oral dryness potentially could impair dietary intake, the literature evaluating the relationship between xerostomia or decreased salivary secretion and dietary intake/nutritional status is sparse and, in addition, mostly concerns elderly populations.
The overall association between salivary flow rate and xerostomia and various nutritional parameters has been studied by the use of malnutrition screening tools like the Mini-Nutritional Assessment Index [2] and the subjective global assessment (SGA) [3] or other anthropometric measurements like body mass index (BMI), triceps skinfold thickness, and mid-arm circumference [4]. These tools are used to identify the state of nutrition and categorize subjects as being well nourished, at risk of malnutrition, or actually malnourished. Thus, studies have shown that xerostomia is significantly more prevalent in subjects at risk of malnutrition and malnourished subjects [5–8]. However, when measuring the actual salivary flow rate, results contradict. Thus, a study measuring both stimulated and unstimulated whole saliva flow rates in a group of Finnish community-dwelling elderly found no association between low unstimulated and stimulated whole saliva flow rates and risk of malnutrition [9], while others report that low stimulated whole saliva flow rates (< 0.7 ml/min) are associated with nutritional deficit in older noninstitutionalized people [10] and that persons with hyposalivation (defined as unstimulated whole saliva flow rates < 0.1 ml/min and stimulated whole saliva flow rates < 0.5 ml/min) present with lower nutritional scores than person with a normal salivary secretion [11]. Concerning the actual dietary intake, the impact of oral dryness has also been studied. Thus, xerostomia in older adults has been associated with inadequate intakes of fiber, potassium, vitamin B6, iron, calcium, and zinc [12], and in patients with Sjögren’s syndrome, the intake of protein, dietary fibers, potassium vitamin A, vitamin C, thiamin, riboflavin, vitamin B6, calcium, iron, and zinc was significantly lower compared with a healthy control group [13]. However, when investigating elderly without xerostomia, comparable deficiencies may be present indicating that elderly generally may be at risk of malnutrition due to other causes than xerostomia and decreased salivary secretion [12]. A study measuring the dietary intake by the healthy eating index (HEI-2005) [14, 15] showed that those with xerostomia were significantly more likely to meet recommendations for total fruit intake (which includes fruit juices) and significantly less likely to meet recommendations for whole-grain products. Additionally, modification of foods has been shown to be more prevalent in the persons with the most severe xerostomia [16]. In a British study including food data based on a list of 16 food items varying from considered easy to difficult to eat, the dietary intake of dentate participants with perceived oral dryness did not seem to be affected, while the edentate participants reported more difficulty to eat the food items that required more chewing [17]. Thus, in general the picture relating dietary intake and salivary secretion is blurred.
Oral Pain and Discomfort
If the salivary deficiency is pronounced, the oral mucosa can appear dry, atrophic, and sometimes inflamed. Major complaints from patients with xerostomia and decreased salivary secretion are a burning sensation, pain and dryness of the mouth, cracking of lips and commissures, and fissuring of the tongue. Additionally, the xerostomic condition is often accompanied by opportunistic microbial infections such as oral candidiasis [18]. Not surprisingly, pain in the mouth due to xerostomia has been associated with malnutrition in a group of institutionalized elderly [8], and in a group of head and neck cancer patients who had been treated with radiotherapy, mucosal sensitivity has been associated with reduced oral energy and protein intake [19].
Challenged Chewing and Swallowing Process
Oral health and comfort is necessary for good masticatory function. Thus, saliva is important in the chewing process, since saliva lubricates food and binds food fragments together in a food bolus which is eventually swallowed. When suffering from decreased salivary secretion, chewing comfort will be diminished, and food will tend to stick to the oral mucosa rather than forming a bolus. Additionally, the swallowing process will be challenged when the lubricating effect of saliva is missing. Accordingly, it has been reported that elderly individuals with xerostomia had difficulty in chewing and swallowing and were significantly more likely to avoid crunchy foods such as carrots and sticky foods such as peanut butter as compared with individuals without xerostomia [20]. These findings are supported in a study investigating mastication, which showed that persons with decreased stimulated parotid saliva flow required twice as many chewing cycles before initial swallowing of two almonds of standardized size as compared with controls with normal salivary flow rate. These dry mouth patients also indicated that their food preferences changed after developing xerostomia. Thus, they reported to cut food into smaller portions and to avoid certain foods such as certain dry breads and foods difficult to chew like carrots [21]. Also, perception of low salivary flow has been associated with poor self-assessed chewing ability [22].
While decreased salivary secretion apparently has some direct impact on chewing ability and dietary intake, one could argue that there is an indirect relation as well. That is because decreased salivary secretion increases the risk of caries [23], which could be followed by loss of teeth, as seen in irradiated head and neck cancer patients [24]. Accordingly, mastication could be impaired, and decreased salivary secretion may therefore indirectly affect dietary intake [25].
To conclude on the association between salivary secretion and dietary intake, it is generally difficult to make unquestionable statements about the impact of salivary gland dysfunction on dietary intake on the basis of the present literature. Depending on the subjects included, which vary between elderly community-dwelling, hospitalized, healthy, and diseased individuals and the methods used for estimating the state of malnutrition or dietary intake, results describe different conditions and situations. However, although the picture is unclear, it is likely that decreased salivary secretion and xerostomia, which could lead to challenged chewing and swallowing, burning, as well as tender oral mucosa, may have a negative impact on dietary intake and nutritional status in some individuals.
Dry Mouth and Sensation of Taste
Saliva contributes to the perception of taste in various ways. Firstly, on the short term, saliva dilutes, digests, or chemically reacts with food stuffs and further transports taste substances to the taste buds and receptors. Secondly, saliva takes part in the long-term maintenance and protection of the taste receptors [26]. Accordingly, decreased salivary secretion and dry mouth may in different ways have an impact on the perception of taste.
The oral taste buds that hold the taste receptor cells are distributed mainly in the oral mucosa although taste buds are also scattered throughout the larynx, pharynx, and epiglottis. In the oral cavity taste buds are primarily situated on the tongue in the foliate and circumvallate papillae but also in the fungiform papillae (Fig. 5.2) and the mucosa of the soft palate. When food is entering the oral cavity, saliva either dilutes, digests, or chemically reacts with food substances and further helps to transport molecules perceived as taste to the taste receptors. Taste sensation is classified into five modalities: sour, sweet, bitter, salt, and umami [27]. Sour taste is primarily caused by acids [28], while a typical sweet stimulus is that of sucrose although other sugars and proteins can also bring about the taste of sweet [29]. The taste of salt classically involves NaCl [30], while bitter taste that is the most sensitive of all taste qualities is caused by both naturally and synthetic compounds, e.g., caffeine, quinine, and strychnine [29].
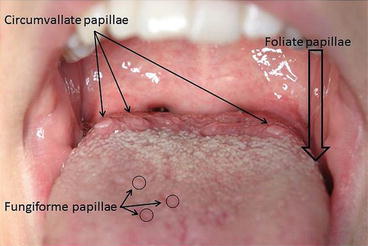
Fig 5.2
A tongue. The papillae that hold taste buds are marked. Around 10–12 circumvallate papillae are located distally on the dorsum of tongue. The fungiform papillae are scattered on the anterior part of the tongue dorsum, while the foliate papillae cannot be seen directly on this picture, since these papillae are situated on the lateral border of the posterior part of tongue. The wide arrow marks the approximate location
Effects of Saliva on Taste Substances
The strongest salivary stimulus is induced by the sour taste modality. It is well known that increased salivary flow rate is associated with a higher bicarbonate concentration and accordingly a higher salivary pH. Bicarbonate is the major buffering ion in stimulated saliva. Since the perception of sour taste is dependent on the presence of H+, an increase in the salivary pH caused by the bicarbonate buffering effect will have a diminishing effect on sour taste perception. Thus, when salivary flow rates were artificially reduced by administration of atropine, the registration threshold of sour taste was lowered [31, 32]. Additionally, higher sour taste threshold has been measured in individuals with higher whole saliva flow rates compared with individuals with lower flow rates [31]. Accordingly, it could be argued that sour taste sensitivity is influenced by salivary flow rate, although the clinical value of this relation needs further investigation.
In addition to salivary bicarbonate, some organic substances in saliva can interact with taste substances. Thus, carbonic anhydrase VI (also named gustin) plays an essential role in taste perception, and a deficiency in this protein has been associated with an overall decreased taste perception [33]. Since carbonic anhydrase VI has been associated with taste bud growth and development, it is suggested that inhibition of synthesis of carbonic anhydrase VI is related to development of taste bud abnormalities followed by loss of taste function [34]. Also, the cyclic nucleotides cAMP and cGMP in parotid saliva have been recognized as playing important roles in maintaining taste function [35], while basic proline-rich proteins and histidine-rich proteins through their binding to polyphenols are involved in the sensation of astringency, which is suggested to be a result of both taste and tactile mechanisms working together [36].
Little is known about the digestive functions of saliva in relation to taste perception. However, the presence of lipase and lipolysis in the oral cavity may play a role in fat perception and liking [37]. The digestion of polysaccharides by amylase starts in the oral cavity [38], and salivary amylase activity may be involved in specific flavor and texture sensations through the enzymatic breakdown of starch [39]. Additionally, the composition of saliva has been associated with the bitter taste sensation [40, 41].
Altered Taste in Dry Mouth Patients
In studies describing clinical characteristics of patients with dry mouth complaints of altered taste are often mentioned [42–44]. Thus, it has been described by several studies that patients with Sjögren’s syndrome present with reduced taste perception [45–47] like irradiated head and neck cancer patients often present with taste alterations [19, 48, 49], although some investigators have observed complete recovery of taste function after 6–12 months after radiation therapy [50]. Concerning the latter group of patients, it has been suggested that loss or alteration of taste may rather be related to the proportion of the tongue contained within the radiation treatment field than the decreased salivary secretion [51]. According to this, there has been described a significant correlation between atrophic tongue mucosa and both salivary flow deficiency and taste function in a group of Sjögren’s syndrome patients [52], which propose that damage to the taste buds or taste receptor sites due to irradiation or decreased salivary secretion additionally may play a role in alterations of taste described in relation to dry mouth.
However, not all patients with xerostomia experience an impaired perception of taste [53]. Likewise, the severity of taste disorder does not necessarily correlate with the degree of parotid and submandibular gland dysfunction [54]. This supports that it is unlikely that the decrease in taste sensitivity can be explained simply by a reduced diffusion of taste substances to the receptor site [55]. While the mixed saliva of the oral cavity is associated with the taste receptors of the fungiform papillae and taste receptors located in the soft palate, the foliate and circumvallate papillae are influenced by flow of von Ebner’s glands [26]. Thus, dysfunction of major salivary glands does not exclude that minor or von Ebner’s salivary glands are still functioning, which could explain that not all patients with xerostomia present with altered taste perception [29].
Regardless of the cause, altered and decreased taste perception is important toward the joy and the actual intake of food. Especially in frail elderly or hospitalized persons with dry mouth, attention should be paid to meal patterns and food intake to prevent inadequate dietary intake. While administration of artificial saliva based on carboxymethylcellulose may have little or no effect on gustatory function [56], it has been shown that flavor enhancement of cooked meals is an effective way to improve dietary intake and body weight in elderly nursing home residents [57].
When evaluating the overall impact of oral dryness and decreased salivary secretion on dietary intake, a prominent example that summarizes the palette of complications is irradiated head and neck cancer patients. These patients experience xerostomia and decreased salivary secretion, oral pain, challenged mastication and swallowing, and altered taste [58], which in many cases lead to a reduced and inadequate dietary intake resulting in an unintended body weight loss [19]. Furthermore, it has previously been described that salivary gland dysfunction may add to the conditions that make it difficult to maintain an adequate dietary intake in elderly populations. Thus, despite the multifactorial etiology of malnutrition in elderly or other individuals suffering from xerostomia and/or decreased salivary secretion, the impact of dry mouth and the concomitant consequences on dietary intake must not be neglected. Therefore, clinical recommendations for counseling individuals suffering from oral dryness should emphasize that this condition may have a negative impact on food consumption behaviors. Hence, questions about altered food choices and amounts as well as recent unintended weight loss may provide relevant anamnestic information in these patients.
The Impact of Nutritional Status on Salivary Secretion
Just as decreased salivary secretion can lead to malnutrition, the opposite can also occur. Thus, persons who live on an unbalanced or inadequate diet may present with xerostomia and/or decreased salivary secretion. Dietary conditions that may prove to have an impact on salivary secretion are dehydration, general malnutrition, and micronutrient deficiencies.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


