History of the Procedure
The maxillectomy was designed for the surgical treatment of tumors involving the maxilla, as well as the maxillary sinus. Lazars attempted the first maxillectomy in 1827, but the procedure was aborted because of excessive blood loss. Later that year, Joseph Gonsol successfully completed this operation but credited Lazars for his initial description of the procedure. In 1829, Syme performed the first successful maxillectomy with orbital exenteration.
The initial attempts at the removal of maxillary tumors resulted in high patient morbidity, including disfigurement and facial scarring. In 1927, Portmann and Rotrouvey described a transoral approach for a maxillectomy. This method provided an additional approach to the maxilla and reduced the need for surgical incisions on the face. This notwithstanding, the greatest risks associated with a maxillectomy included postoperative wound infection and extensive blood loss. In the 1950s, significant advancements in anesthetic techniques helped to reduce intraoperative blood loss, thus decreasing the patient morbidity and mortality often seen with this procedure. During this time, the Weber-Ferguson approach to the maxillectomy was described, which eliminated a deforming scar while still providing excellent access to the midfacial skeleton.
Advancements in surgical techniques and improved instrumentation have allowed for a less invasive approach to some maxillary tumors. In 1977, Sessions and Larson described the medial maxillectomy for lesions of the lateral nasal wall. Later on, with the development of the nasal endoscope, smaller lesions extending from the lateral nasal wall could be removed with improved visualization. The maxillectomy procedure has continued to evolve, while both improving patient outcomes and decreasing complications.
History of the Procedure
The maxillectomy was designed for the surgical treatment of tumors involving the maxilla, as well as the maxillary sinus. Lazars attempted the first maxillectomy in 1827, but the procedure was aborted because of excessive blood loss. Later that year, Joseph Gonsol successfully completed this operation but credited Lazars for his initial description of the procedure. In 1829, Syme performed the first successful maxillectomy with orbital exenteration.
The initial attempts at the removal of maxillary tumors resulted in high patient morbidity, including disfigurement and facial scarring. In 1927, Portmann and Rotrouvey described a transoral approach for a maxillectomy. This method provided an additional approach to the maxilla and reduced the need for surgical incisions on the face. This notwithstanding, the greatest risks associated with a maxillectomy included postoperative wound infection and extensive blood loss. In the 1950s, significant advancements in anesthetic techniques helped to reduce intraoperative blood loss, thus decreasing the patient morbidity and mortality often seen with this procedure. During this time, the Weber-Ferguson approach to the maxillectomy was described, which eliminated a deforming scar while still providing excellent access to the midfacial skeleton.
Advancements in surgical techniques and improved instrumentation have allowed for a less invasive approach to some maxillary tumors. In 1977, Sessions and Larson described the medial maxillectomy for lesions of the lateral nasal wall. Later on, with the development of the nasal endoscope, smaller lesions extending from the lateral nasal wall could be removed with improved visualization. The maxillectomy procedure has continued to evolve, while both improving patient outcomes and decreasing complications.
Indications for the Use of the Procedure
The primary indication for maxillectomy is ablation of malignant and specific benign diagnoses. Additional indications for maxillectomy include advanced fungal disease such as mucormycosis and aspergillosis, bisphosphonate osteonecrosis, and osteoradionecrosis. Variations of the maxillectomy include the extraoral approach via a Weber-Ferguson incision. It is the purpose of this chapter to describe the indications, limitations, and technique for maxillectomy for benign disease.
Resection margins for locally aggressive benign odontogenic lesions such as ameloblastoma or myxoma traditionally include 1 cm of bone and one intact anatomic barrier. The periosteum and the overlying mucosa may be preserved if the lesion is contained within the maxilla and has not extended beyond the confines of the bone. However, tumors that have perforated the maxilla require sacrifice of the adjacent overlying periosteum.
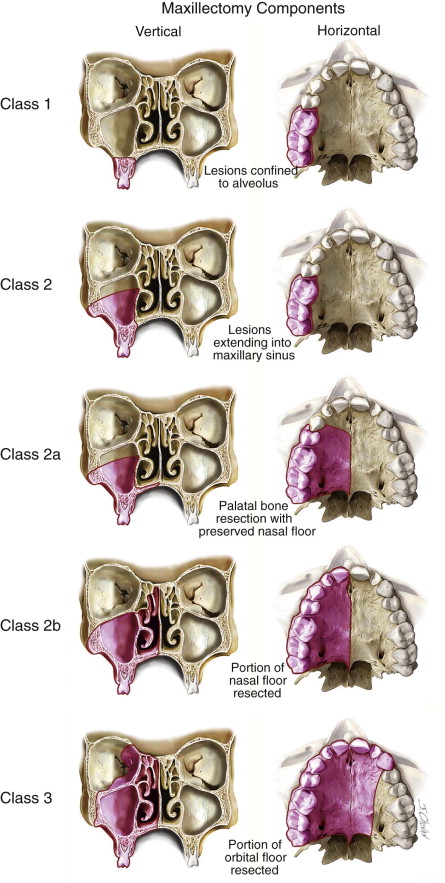
The extent of the resection is dependent on the histologic diagnosis as well as the size and location of the neoplasm. The Brown classification system provides a useful method for planning the maxillectomy and for defining the reconstructive options. For lesions confined to the alveolus, a Brown Class I maxillectomy defect would be anticipated ( Figure 84-1 ). This type of maxillectomy does not result in an oral-antral or oral-nasal communication. For benign neoplasms that extend into the maxillary sinus, a higher-level resection, including the maxillary sinus walls, would be indicated, resulting in a Brown Class 2 defect. Additionally, the horizontal margin of the resection must also be considered. Unilateral lesions often require resection of a portion of the palatal bone but not the nasal floor (Brown Class 2a). More extensive or anterior lesions may require sacrifice of a portion of the nasal floor (Brown Class 2b). Lastly, advanced neoplastic disease with extension to the orbital floor may require resection of the orbital floor (Brown Class III). This type of maxillectomy requires additional exposure in the form of a Weber-Ferguson incision.
Limitations and Contraindications
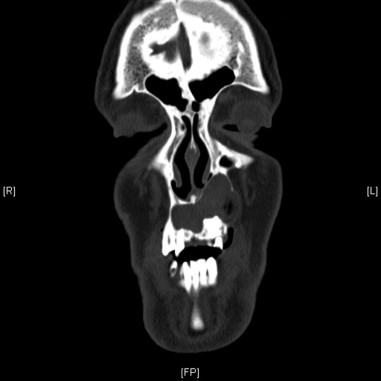
Limitations of the maxillectomy technique are primarily due to anatomic features of the individual lesion, as indicated previously. Careful preoperative radiographic evaluation in all three planes is required, with particular attention to possible extension beyond the confines of the maxilla in the region of the nasal floor, orbital floor, and posterior maxilla ( Figures 84-2 to 84-4 ). There are no specific contraindications to maxillectomy.


Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


