Armamentarium
|
History of the Procedure
An ancient text from Egypt, written around 1600 bc , is kept in a vault at the New York Academy of Medicine. This papyrus was copied from an even older version dating back to 3000 bc . It contains information on 48 surgical cases and includes well-described clinical observations. The document is called the Edwin Smith papyrus, or the “ book of wounds.” Edwin Smith was a nineteenth-century American archaeologist who purchased the papyrus from an antiquities dealer in Luxor in 1862. The papyrus, which was translated after Smith’s death, has expanded our knowledge of the history of ancient surgery.
The Egyptians were the first culture to describe sutures. The technique of suturing was used in the embalming of corpses after evisceration of the body organs. Sutures can be seen in mummies dating back to 1100 bc . The first description of cautery was recommended by the Egyptians to control hemorrhage. Boiling oil was applied to the bleeding wound in an attempt to cauterize it. It has been shown that in ancient India, physicians practiced suturing between 800 and 600 bc . The materials they described were cotton thread, hemp, strips of horsehair, leather, and animal tendons. At that time, the Indian physician Susruta described four wound classes, incised, contused, crushed, and torn. This corresponds to the wounds we see today. Incised wounds result from sharp-edged objects passed through the skin. Lacerations, on the other hand, occur when the skin is torn open by blunt force trauma. Susruta recommended removing all foreign bodies from a wound and believed that infected wounds should not be closed. Later, the ancient Greeks noticed that facial wounds healed faster than extremity wounds. They reserved sutures for fast-healing wounds and left large wounds open for “suppuration.” Hippocrates (460-377 BC), the “father of medicine,” wrote that wounds should be clean and dry and that surgeons should wash their hands. Our ancestors were well aware that wounds healed differently under certain conditions. They observed that wound edges in close proximity healed faster than wounds that gaped; this is the principle of healing by primary or secondary intention. The Roman physician Celsus ( ad 25-50) described this and the technique of using ligatures to tie off blood vessels. Celsus also invented a small artery forceps and used the tourniquet technique on limb wounds. Other enormous contributions to the developing science of surgery were made by Galen, Paré, Pasteur, Lister, and Kocher.
The contributions of William S. Halsted (1852-1922) cannot be overemphasized in the discussion of the history of American surgery. Halsted had been a student of Theodor Billroth (1829-1894) in Vienna, Austria. After traveling Europe, Halsted became instrumental in developing a German model of formalized, rigorous surgical residency training in the United States. At the newly opened Johns Hopkins Hospital, Halsted revolutionized surgery with the use of rubber gloves, aseptic operating room (OR) conditions, and waterproof surgical gowns. Halsted’s basic surgical principles were the gentle handling of tissues, careful hemostasis, and appropriate irrigation of wounds. Sir Harold Gilles (1882-1960), a New Zealand–born otolaryngologist, was influential in developing the specialty of plastic surgery. In England, Gilles treated thousands of facial injuries during and after World War I. He published his techniques and results in the landmark text Plastic Surgery of the Face in 1920.
History of the Procedure
An ancient text from Egypt, written around 1600 bc , is kept in a vault at the New York Academy of Medicine. This papyrus was copied from an even older version dating back to 3000 bc . It contains information on 48 surgical cases and includes well-described clinical observations. The document is called the Edwin Smith papyrus, or the “ book of wounds.” Edwin Smith was a nineteenth-century American archaeologist who purchased the papyrus from an antiquities dealer in Luxor in 1862. The papyrus, which was translated after Smith’s death, has expanded our knowledge of the history of ancient surgery.
The Egyptians were the first culture to describe sutures. The technique of suturing was used in the embalming of corpses after evisceration of the body organs. Sutures can be seen in mummies dating back to 1100 bc . The first description of cautery was recommended by the Egyptians to control hemorrhage. Boiling oil was applied to the bleeding wound in an attempt to cauterize it. It has been shown that in ancient India, physicians practiced suturing between 800 and 600 bc . The materials they described were cotton thread, hemp, strips of horsehair, leather, and animal tendons. At that time, the Indian physician Susruta described four wound classes, incised, contused, crushed, and torn. This corresponds to the wounds we see today. Incised wounds result from sharp-edged objects passed through the skin. Lacerations, on the other hand, occur when the skin is torn open by blunt force trauma. Susruta recommended removing all foreign bodies from a wound and believed that infected wounds should not be closed. Later, the ancient Greeks noticed that facial wounds healed faster than extremity wounds. They reserved sutures for fast-healing wounds and left large wounds open for “suppuration.” Hippocrates (460-377 BC), the “father of medicine,” wrote that wounds should be clean and dry and that surgeons should wash their hands. Our ancestors were well aware that wounds healed differently under certain conditions. They observed that wound edges in close proximity healed faster than wounds that gaped; this is the principle of healing by primary or secondary intention. The Roman physician Celsus ( ad 25-50) described this and the technique of using ligatures to tie off blood vessels. Celsus also invented a small artery forceps and used the tourniquet technique on limb wounds. Other enormous contributions to the developing science of surgery were made by Galen, Paré, Pasteur, Lister, and Kocher.
The contributions of William S. Halsted (1852-1922) cannot be overemphasized in the discussion of the history of American surgery. Halsted had been a student of Theodor Billroth (1829-1894) in Vienna, Austria. After traveling Europe, Halsted became instrumental in developing a German model of formalized, rigorous surgical residency training in the United States. At the newly opened Johns Hopkins Hospital, Halsted revolutionized surgery with the use of rubber gloves, aseptic operating room (OR) conditions, and waterproof surgical gowns. Halsted’s basic surgical principles were the gentle handling of tissues, careful hemostasis, and appropriate irrigation of wounds. Sir Harold Gilles (1882-1960), a New Zealand–born otolaryngologist, was influential in developing the specialty of plastic surgery. In England, Gilles treated thousands of facial injuries during and after World War I. He published his techniques and results in the landmark text Plastic Surgery of the Face in 1920.
Indications for the Use of the Procedure
In the repair of facial lacerations, we must be concerned with both the skin and what lies beneath. Deep wounds may damage nerves, blood vessels, salivary glands/ducts, muscle, bone, or the globe ( Figure 58-1 ). Penetration into various body cavities or sinuses can also occur. Reconstruction of a soft tissue injury is performed for two reasons: to restore the function of the damaged part and to restore its physical form.
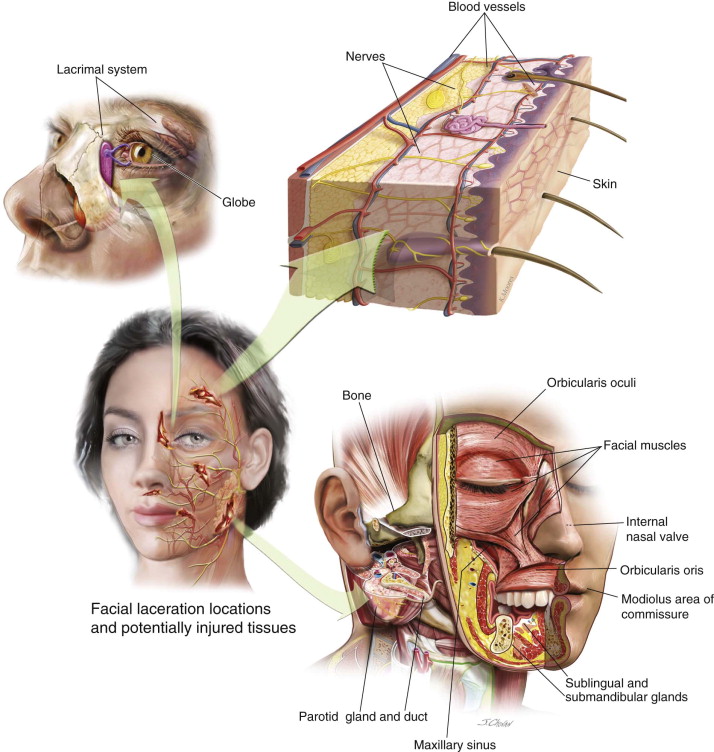
Special functions in the face include opening and closing the eyes. Thus, the status of both the orbicularis oculi and levator palpebrae muscles should be assessed. A functioning lacrimal system is needed to prevent epiphora. Moving the muscles of the face is important for us to communicate and express ourselves. Parotid gland secretory function requires a patent duct from the gland to the oral cavity. Nasal respiration is important to warm, humidify, and clean the air before it gets to the lungs. Nasal stenosis or adhesions after laceration can obliterate the internal nasal valve. This precludes nasal respiration on the affected side. Orbicularis oris function is important to provide a competent oral seal. Lacerations to the modiolus area of the commissure may produce microstomia, limiting oral hygiene and dental care.
The second important reason to intervene is to restore the physical form of the face. Prominent scars can have a profound effect upon self-esteem and psychological well-being. Unfortunately for humans, skin as a composite tissue heals by repair, not by regeneration. Only the epithelium of the skin regenerates. Therefore, scarring through the dermis is inevitable.
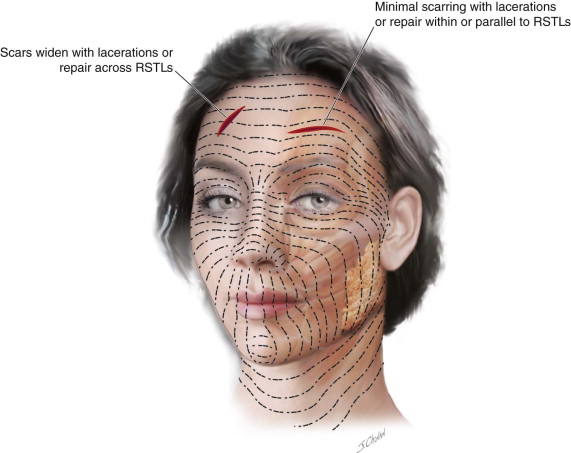
Unlike elective incisions, we cannot control the direction of a facial laceration. An important concept to understand in both elective incisions and lacerations is the principle of relaxed skin tension lines (RSTLs) ( Figure 58-2 ). Lacerations that parallel the RSTLs or fall in natural skin creases generally produce a more cosmetically appealing scar. Scars tend to widen if they cross the RSTLs. Therefore, it is important to provide good dermal support in the closure, especially when lacerations cross the RSTLs. Tension should not be placed on the superficial skin sutures. Irregular lacerations should be excised (minimally) in an attempt to produce a linear scar. The ultimate goal is to produce the narrowest, flattest, most inconspicuous scar possible.
Limitations and Contraindications
Facial wounds should be repaired primarily in nearly all situations. Early closure of the well-vascularized facial tissues allows healing by primary intention. (Avulsive facial wounds are not covered in this chapter.) When there is damage to underlying structures, a short period can be observed before wound closure without the increased risk of infection, provided the wound is cleaned and dressed appropriately. Exposure of facial fractures through the laceration should always be attempted so that additional facial incisions can be avoided.
Contaminated or infected wounds are managed differently. If there has been a significant delay in presentation to the emergency department (ED), open wounds can become colonized with the native flora. Staphylococcus epidermidis is a normal skin flora that can gain access once the skin has been violated. Traumatic wounds can also have Streptococcus pyogenes and Staphylococcus aureus present. Contaminated wounds can be closed primarily if decontamination is performed. (Irrigation and débridement are discussed in the following technique.) If devitalized tissue and foreign bodies are present in the wound, fewer bacterial organisms are necessary to cause a wound infection. The only contraindication to primary closure of lacerations is the presence of gross infection. In this situation, the laceration should be packed, changed regularly. and finally closed by tertiary intention (i.e., delayed primary closure).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


