Instability following orthodontic tooth movement has been a recurring problem for the practicing orthodontist and the profession. Many dental professionals who see such patients later assume incompetence on the part of the treating orthodontist.
Treatment of diastemas is common after space closure ( Fig. 18-l ). Many orthodontists view permanent retention as the only realistic approach to maintaining closure ( Fig. 18-2 ). Removable appliances used for retention create back-and-forth movement as a result of being worn “on and off” ( Fig. 18-3 ). Although many orthodontists resort to frenectomies and circumferential fibrotomies, the outcome in these cases is often frustrating because undesirable side-effects still occur. Thus, even with surgical procedures, some form of retention is frequently required.



ARCHWIRE REMOVAL AND CLINICIAN CONCERNS
This chapter addresses an approach used by the author for many years in which all archwires are removed during treatment as a mandatory phase of orthodontic tooth movement. This approach has a better than 90% success rate. Such wires are removed for at least 6 weeks, but often longer as situations demand (e.g., summer vacation). This does not mean, however, that archwires must be removed for every type of instability, such as crossbites, open bites, overbites, and rotations. These different areas may be checked for stability versus instability at the same time. Common sense prevails in this regard; treatment time should not be extended because of archwire removal.
The typical orthodontist resists removing archwires during orthodontic treatment because of possibly losing some of the movement achieved. It is for this very reason, however, that archwires are removed. Teeth “rebound” for several reasons, but in any case will attempt to put themselves into equilibrium with muscles and function. Cephalometrics may encourage the placement of teeth in certain anteroposterior as well as transverse positions. However, the numbers and angles involved do not apply to each patient treated, but rather to a collection of such patients.
Averages can be misleading when individualizing tooth movement for the patient. If a clothing store carried only trousers with the average size for men, theoretically there might not be a single pair of trousers that fits any of them. Although unlikely, this illustrates that the best “fit” for the patient is one that has been “tailor-made” for the individual in question. This means recognizing that tooth position is determined by muscles, function, and habits, along with duration and related factors.
But how can all this be achieved? There must be a better way than the traditional approach, associated with such a high degree of failure in the absence of permanent retention.
All orthodontists are aware of cause-and-effect relationships. However, not all orthodontists necessarily ask, “Why?” when observing undesirable outcomes, and instead frequently resort to some type of appliance, laboratory or otherwise, to resolve the problem. In other words, treatment often involves treating the “effect” rather than the cause.
“GEDANKEN” EXPERIMENT
In attempting to solve the problem of stabilizing diastema closure without permanent retention, the author decided to use the same approach that Einstein used so successfully when arriving at a number of still-valid scientific facts. Einstein was often criticized for creating experiments in his mind without actually performing them; he became famous for his Gedanken (“thought”) experiments. This frustrated his fellow scientists, who believed that validating results required actual experiments.
In using a “gedanken experiment” to try and resolve the diastema problem, the author first needed to ask the following question: “Do we know of any other situations in orthodontic tooth movement that result in the creation of space following space closure?” One answer would be the space opening orthodontists frequently witness after space closure in a four first-bicuspid extraction case for adults ( Fig. 18-4 ). As a “thought” experiment only, one can visually ask, if the space readily reopened after paralleling of the roots, what might happen if the crowns were severely tipped toward each other, instead of paralleling the roots? Obviously, this would create serious periodontal problems and would not be considered a solution, but only a mental experiment. However, one could still conclude (without actually doing it) that the greater the tipping, the greater the probability of increased stability following space closure. The logical question would then be, “Why?”
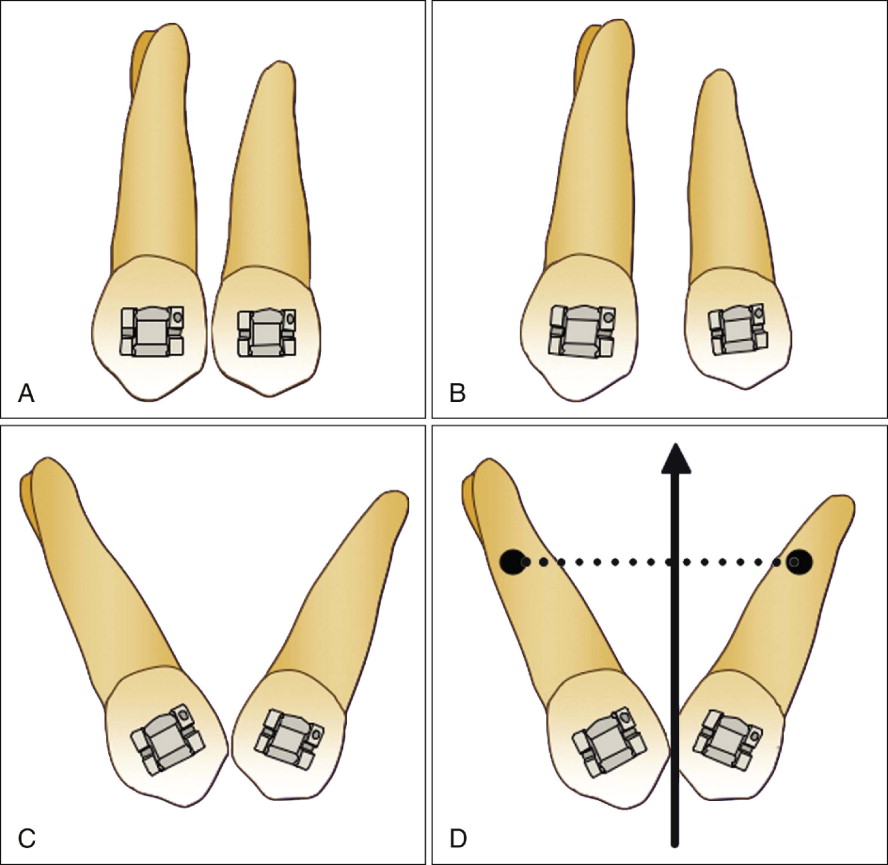
As can be seen in Fig. 18-5 , the occlusal forces acting on the cuspid and bicuspid would take place through a greater perpendicular distance from the centers of resistance in these teeth, thus creating so-called functional moments. Also, if the central incisors were observed with the same angular displacement as shown with the cuspid and bicuspid, the incisal forces would produce the same increased “functional moments,” for the same reason. Although with the central incisors the angular displacement would require primarily root displacement, it is the increased separation of the centers of resistance that results in these functional moments.
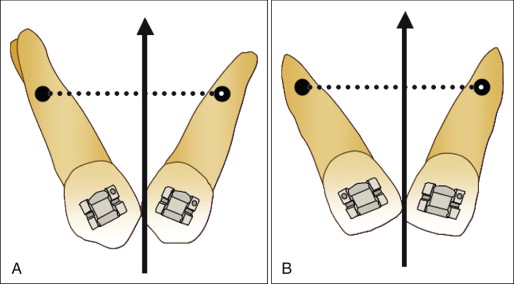
Although diverging the roots to this extent would never be considered, in this gedanken experiment one can reasonably conclude that stability lies somewhere between these two extremes. This mental experiment provides the knowledge that “somewhere” there is stability when the centers of resistance have been sufficiently displaced during such exaggerated tooth inclination. It now remains to be discovered whether such change in inclination remains within acceptable limits for the patient.
In the case of a diastema, the central incisor crowns can only move together until contact is made, at which time the remaining movement consists of only distal movement of the central incisor roots. Any time a moment is applied to teeth—whenever crown movement is prevented in one direction—root movement occurs in the opposite direction. This is demonstrated many times as this experiment progresses.
“GEDANKEN” EXPERIMENT
In attempting to solve the problem of stabilizing diastema closure without permanent retention, the author decided to use the same approach that Einstein used so successfully when arriving at a number of still-valid scientific facts. Einstein was often criticized for creating experiments in his mind without actually performing them; he became famous for his Gedanken (“thought”) experiments. This frustrated his fellow scientists, who believed that validating results required actual experiments.
In using a “gedanken experiment” to try and resolve the diastema problem, the author first needed to ask the following question: “Do we know of any other situations in orthodontic tooth movement that result in the creation of space following space closure?” One answer would be the space opening orthodontists frequently witness after space closure in a four first-bicuspid extraction case for adults ( Fig. 18-4 ). As a “thought” experiment only, one can visually ask, if the space readily reopened after paralleling of the roots, what might happen if the crowns were severely tipped toward each other, instead of paralleling the roots? Obviously, this would create serious periodontal problems and would not be considered a solution, but only a mental experiment. However, one could still conclude (without actually doing it) that the greater the tipping, the greater the probability of increased stability following space closure. The logical question would then be, “Why?”
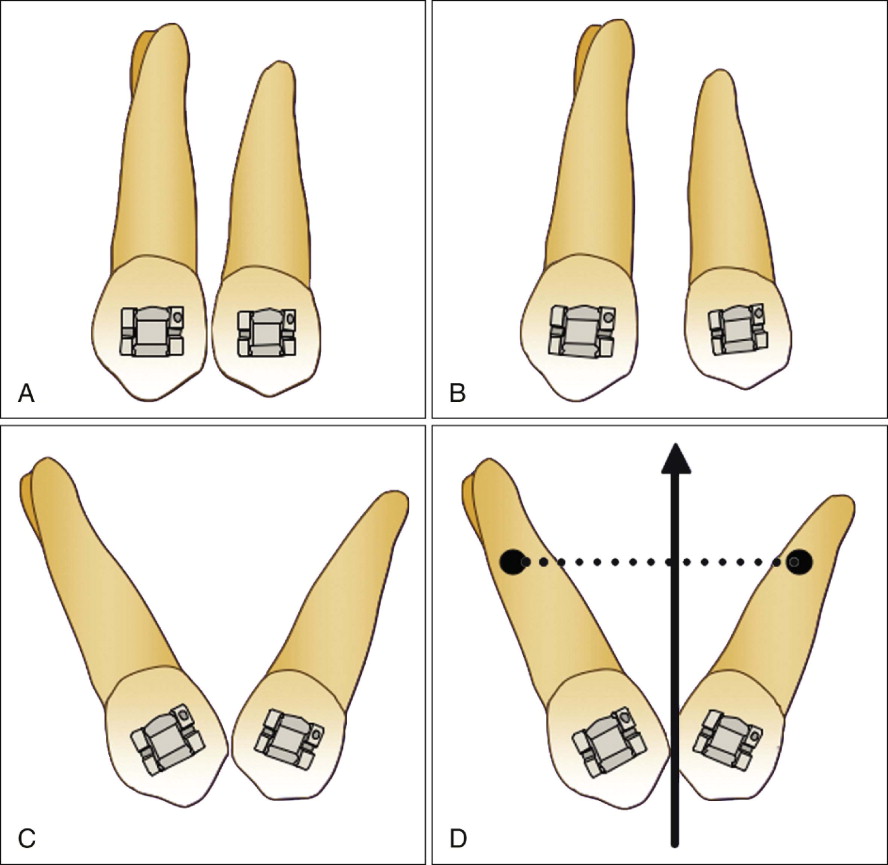
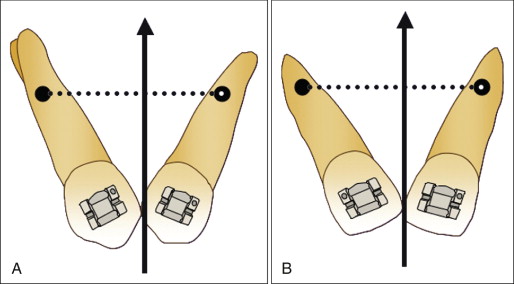
As can be seen in Fig. 18-5 , the occlusal forces acting on the cuspid and bicuspid would take place through a greater perpendicular distance from the centers of resistance in these teeth, thus creating so-called functional moments. Also, if the central incisors were observed with the same angular displacement as shown with the cuspid and bicuspid, the incisal forces would produce the same increased “functional moments,” for the same reason. Although with the central incisors the angular displacement would require primarily root displacement, it is the increased separation of the centers of resistance that results in these functional moments.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


