P atients with open bite often complain of functional disorders, such as difficulties in cutting and chewing food with the upper and lower incisors ( Fig. 14-1 ), as well as speech difficulty. Clinicians need to understand the factors causing this dentofacial skeletal problem and design therapeutic solutions accordingly.
CLASSIFICATION OF OPEN BITE
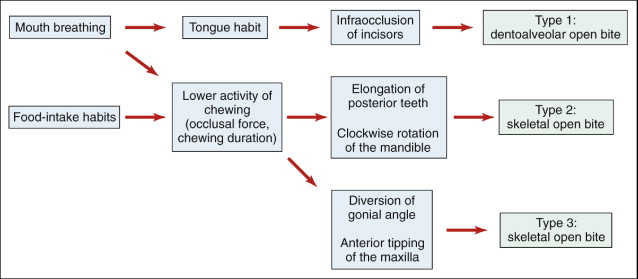
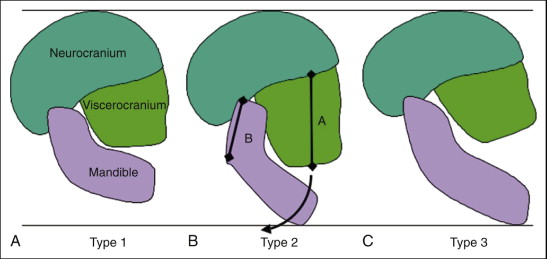
There are three types of open bite ( Fig. 14-2 ). The finger-sucking habit during childhood impedes normal eruption of the anterior teeth and alveolar growth and induces dentoalveolar open bite. Prevention of the deleterious habit should be helpful in improving this type of open bite. Skeletal open bite with a long face can be divided into two types, one caused by clockwise rotation of the mandible, and the other by skeletal deformation, such as tipping of the maxilla and diversion of the gonial angle of the mandible.
Open bite is always accompanied by a tongue-thrusting habit. It appears that individuals with a long face have weaker contraction of the mandibular elevator muscles, lower electromyographic (EMG) activity of the muscles during maximum voluntary clenching, and lower occlusal force than the corresponding values of short-face individuals.
Mechanisms of Skeletal Open Bite
The main mechanism responsible for skeletal open bite is a proportional discrepancy between the anterior and posterior facial heights. The vertical height of the nasomaxillary complex, the ramus height, and the posterior teeth are important factors that determine the mandibular vertical position. Any elongation or extrusion of the posterior teeth will result in a clockwise rotation of the mandible (see Fig. 14-2 ).
MASTICATION AND VERTICAL POSITION OF POSTERIOR TEETH
Magnitude and duration of force application are important factors for the stability of tooth position. The occlusal contact and the eruptive or extrusive movement of the tooth determine the vertical position of the posterior teeth. The magnitude of tooth contact force on the posterior teeth depends on the strength of muscular activity. The duration of daily tooth contact varies between 1 and 3 hours, depending on the duration of mastication, swallowing, and sleeping.
Unless the magnitude and duration of occlusal contact force are sufficient to prevent elongation of the posterior teeth, they will extrude, resulting in open bite. For example, the food features or the food-intake habits of young people, such as consumption of soft diet within a short eating time and irregular meal intake, could result in reduced tooth contact of the posterior teeth and subsequent development of vertical occlusal problems.
The author’s investigation was based on a questionnaire for dental students age 18 to 26 years. It showed that 55% of male and 81% of female students regularly eat three meals a day. Male students reported spending 48.1 minutes and female students 60.0 minutes eating food over three meals ( Table 14-1 ).
| Breakfast (min) | Lunch (min) | Dinner (min) | Total Time (min) | |
|---|---|---|---|---|
| Male ( n = 49) | 7.6 | 18.8 | 21.8 | 48.1 |
| Female ( n = 49) | 11.5 | 21.2 | 27.3 | 60.00 |
| mean ( n = 76) | 8.8 | 19.3 | 23.2 | 51.4 |
Taking these findings into consideration, one can hypothesize that intensifying the vertical effect on the posterior teeth by increasing the degree and duration of the occlusal contact is a useful strategy (1) to promote healthy development of occlusion in growing children and (2) to obtain a stable outcome after orthodontic or orthognathic treatment.
Several studies have described methods to intensify muscle activity based on isometric muscle exercise. As reported by several investigators, isometric clenching increases the contraction force of the elevator muscle of the mandible and the bite force on the posterior teeth. Some studies were done to examine only the muscular activity and bite force. Muscle exercise was used to intensify the vertical effects on the teeth by increasing the magnitude and duration of the occlusal contact.
Clenching Exercise Using Soft Bite Block
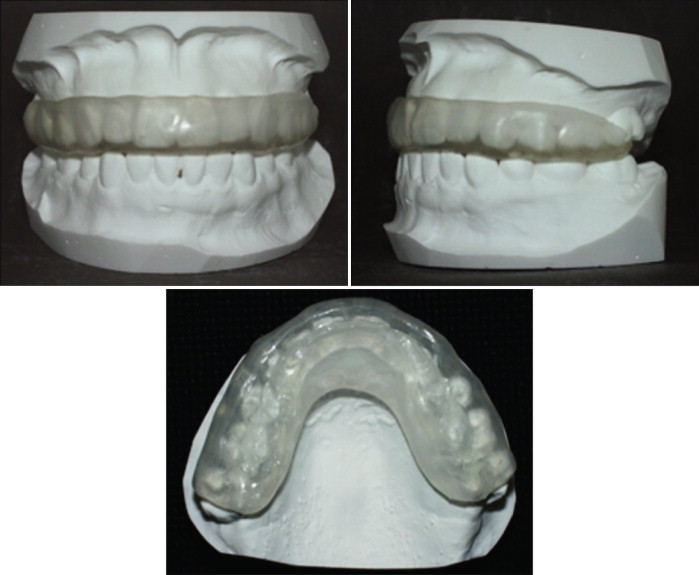
In one study, 24 healthy adult volunteers performed isometric clenching at maximum voluntary contraction against a soft bite block for 3 seconds with 5 seconds of rest over a 15-minute session, with at least two sessions per day over 8 weeks ( Fig. 14-3 ). The occlusal contact area and pressure were recorded using Dental Prescale film and analyzed by the Occluzer (FPD 703, Fuji Film, Tokyo, Japan). The upper soft bite block was adjusted to make full contact with the lower teeth in a nonrestrained mandibular position, to prevent negative reflection caused by possible interference of a single tooth.
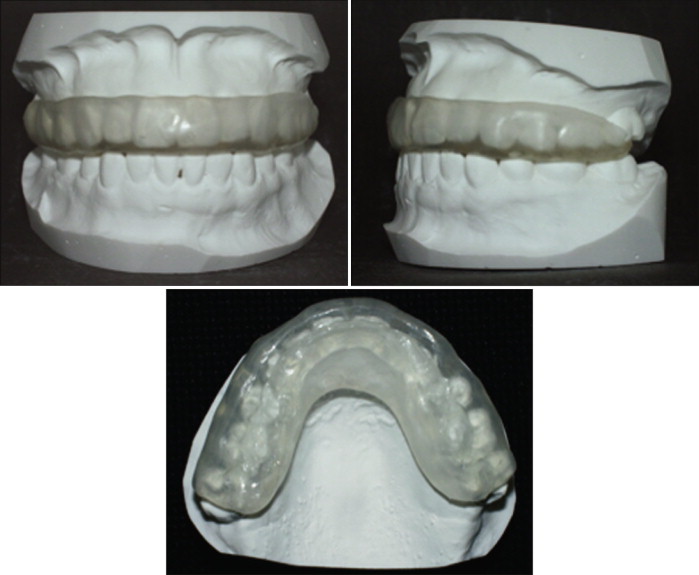
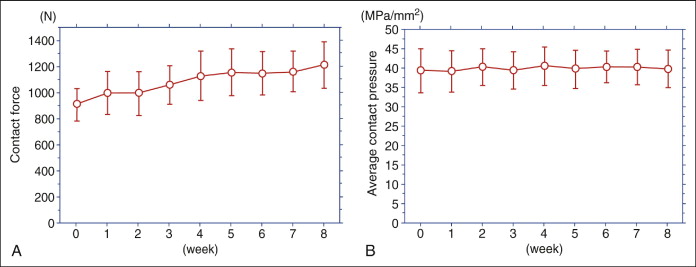
Subjects who complained about discomfort on the dentition and temporomandibular joint during muscle training were excluded from the study. It was presumed that the contact pressure during clenching the bite block at voluntary contraction was equivalent to the pressure on biting a Dental Prescale sheet. Although the occlusal parameters, including occlusal contact area and occlusal force, were higher in men than in women, the total contact force was 1122 ± 398 newtons (N), and the average contact pressure was 35.9 ± 4.7 megapascals (MPa)/mm 2 at baseline ( Table 14-2 ). Therefore the degree of occlusal contact force on the posterior teeth during clenching the bite block was more than the optimal force for tooth movement. The vertical force on the posterior teeth was not continuous but intermittent.
| Occlusal Force (N) | Occlusal Contact Area (mm 2 ) | Occlusal Pressure (MPa/ mm 2 ) | |
|---|---|---|---|
| Men | 1223.7 | 35.2 | 35.8 |
| Women | 895.8 | 26.99 | 36 |
| total | 1122.2 | 32.6 | 35.9 |
With regard to the duration of the muscle-training program, Petrofsky and Laymon reported an effective training protocol that involved electrical stimulation of the quadriceps muscles, in which training was conducted for 15 or 30 minutes each day. Thompson et al. stated that isometric clenching against a soft maxillary splint for five 1-minute sessions per day over a 6-week period increased the maximum bite force. Tzakis et al. studied the influence of 30 minutes of intense chewing for 5 days on the masticatory function and showed that such a protocol had variable short-term effects on masticatory function. Kihara reported that the average time of daily tooth contact at the first molar was 67 minutes, and that the mean frequency of daily tooth contact was about 4270 times in normal adult men.
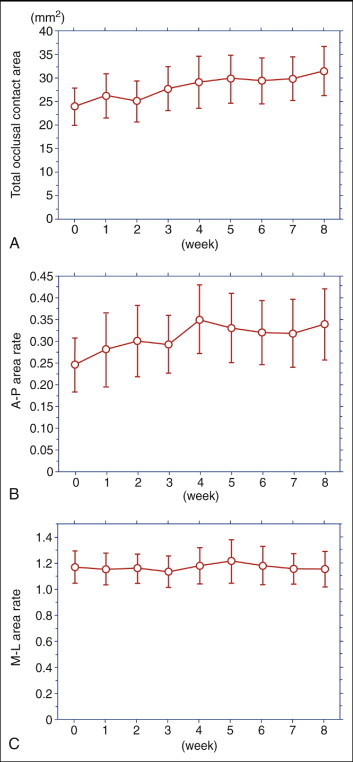
It seems that isometric clenching on a bite plate for 30 minutes a day over 8 weeks prolongs the time of tooth contact and intensifies the vertical effect on dentition. In a preliminary study, the author’s group found that it was very difficult for subjects to clench their teeth persistently over 30 minutes every day over 1 week. Instead, the subjects were asked to perform isometric clenching at maximum voluntary contraction against a soft bite block for 3 seconds with 5 seconds’ rest for 15-minute sessions, with at least two sessions per day over 8 weeks. Recording of occlusal parameters was repeated three times with 3-minute intervals, and repeated over 5 days in the control group and every week for 8 weeks in the exercise group. This protocol increased the total, anterior, and posterior occlusal contact areas to 135.8%, 219.8%, and 129.6% relative to the baseline values, respectively, following the 8-week exercise ( Fig. 14-4, A ), and also significantly increased the anteroposterior balance of occlusal contact area ( Fig. 14-4, B ). The same 8-week exercise did not alter the mesiolateral balance of occlusal contact area ( Fig. 14-4, C ) or the contact pressure ( Fig. 14-5 ).
Chewing Gum Exercise
The author’s results indicated that isometric muscle exercise for 8 weeks increased occlusal contact area and advanced the balance of occlusal contact area. The questionnaire study on muscle exercise using a soft bite plate revealed that it was very difficult for subjects to continue the clenching exercise using the soft bite plate for 8 weeks. It was necessary to find a more comfortable and effective exercise protocol.
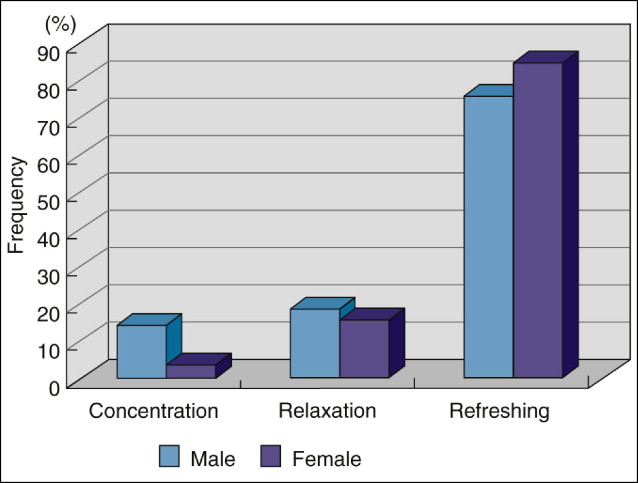
The habit of chewing gum is popular in many countries, especially after the introduction of sugarless chewing gum. The most frequent answer to the question, “What do you think is the purpose of chewing a gum?” was that chewing a gum was refreshing, enhanced concentration, and released stress ( Fig. 14-6 ). These findings indicated that chewing gum is not a stressful but rather a stress-releasing habit.
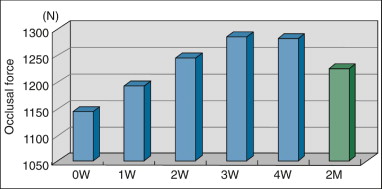
Because a more comfortable training protocol is more likely to be continued, the “chewing gum exercise” was designed. This involved chewing gum for 30 to 45 minutes per day over 4 weeks. Fifty dental students were enrolled in this study. The same occlusal parameters were estimated at the end of the exercise and 1 month later. At the end of the chewing gum exercise, the total occlusal force increased to 140% ( Fig. 14-7 ), total contact area increased to 125%, but the occlusal pressure remained the same, relative to baseline values (before the exercise). One month after the end of the exercise, the increased occlusal force and occlusal contact area decreased to 105% and 103% of baseline, respectively.
These results suggest that the chewing gum exercise is effective in increasing the occlusal contact and occlusal force. In addition, at the end of the protocol, most of the subjects answered “yes” to the question, “Do you think masticatory exercise using a chewing gum is comfortable to continue the training program?”
Preserving Vertical Effect on Posterior Teeth after Correction of Open Bite
In the treatment of open bite or edge-to-edge bite, intrusion of the posterior teeth or maintenance of the posterior occlusal height is usually achieved by increasing the vertical effect on the posterior teeth using high-pull headgear, bite block, or metal implant. Unless the magnitude and duration of occlusal contact force is sufficient to prevent elongation of the posterior teeth after active treatment, the posterior teeth will extrude again and result in recurrence of the open bite. This makes it imperative to preserve the vertical effect on the posterior teeth after active orthodontic and orthognathic surgical treatment of the open bite. The “chewing gum exercise” is one method that can ensure long-term stability in such patients.
MASTICATION AND VERTICAL POSITION OF POSTERIOR TEETH
Magnitude and duration of force application are important factors for the stability of tooth position. The occlusal contact and the eruptive or extrusive movement of the tooth determine the vertical position of the posterior teeth. The magnitude of tooth contact force on the posterior teeth depends on the strength of muscular activity. The duration of daily tooth contact varies between 1 and 3 hours, depending on the duration of mastication, swallowing, and sleeping.
Unless the magnitude and duration of occlusal contact force are sufficient to prevent elongation of the posterior teeth, they will extrude, resulting in open bite. For example, the food features or the food-intake habits of young people, such as consumption of soft diet within a short eating time and irregular meal intake, could result in reduced tooth contact of the posterior teeth and subsequent development of vertical occlusal problems.
The author’s investigation was based on a questionnaire for dental students age 18 to 26 years. It showed that 55% of male and 81% of female students regularly eat three meals a day. Male students reported spending 48.1 minutes and female students 60.0 minutes eating food over three meals ( Table 14-1 ).
| Breakfast (min) | Lunch (min) | Dinner (min) | Total Time (min) | |
|---|---|---|---|---|
| Male ( n = 49) | 7.6 | 18.8 | 21.8 | 48.1 |
| Female ( n = 49) | 11.5 | 21.2 | 27.3 | 60.00 |
| mean ( n = 76) | 8.8 | 19.3 | 23.2 | 51.4 |
Taking these findings into consideration, one can hypothesize that intensifying the vertical effect on the posterior teeth by increasing the degree and duration of the occlusal contact is a useful strategy (1) to promote healthy development of occlusion in growing children and (2) to obtain a stable outcome after orthodontic or orthognathic treatment.
Several studies have described methods to intensify muscle activity based on isometric muscle exercise. As reported by several investigators, isometric clenching increases the contraction force of the elevator muscle of the mandible and the bite force on the posterior teeth. Some studies were done to examine only the muscular activity and bite force. Muscle exercise was used to intensify the vertical effects on the teeth by increasing the magnitude and duration of the occlusal contact.
Clenching Exercise Using Soft Bite Block
In one study, 24 healthy adult volunteers performed isometric clenching at maximum voluntary contraction against a soft bite block for 3 seconds with 5 seconds of rest over a 15-minute session, with at least two sessions per day over 8 weeks ( Fig. 14-3 ). The occlusal contact area and pressure were recorded using Dental Prescale film and analyzed by the Occluzer (FPD 703, Fuji Film, Tokyo, Japan). The upper soft bite block was adjusted to make full contact with the lower teeth in a nonrestrained mandibular position, to prevent negative reflection caused by possible interference of a single tooth.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


