Most orthodontic cases feature a shortage of space and some crowding. Although nonextraction treatment has become popular in the last decade, many patients still require treatment based on tooth extraction.
The first phase of treatment in premolar extraction cases is distalization of the canines. Using conventional orthodontic techniques, biological tooth movement can be achieved at a limited rate. The canine retraction phase usually lasts about 6 to 8 months. In addition, extraoral or intraoral anchorage mechanics are required to keep the obtained space safe during canine distalization, particularly when maximum or moderate anchorage is required. Therefore, under normal circumstances, conventional treatment with fixed appliances is likely to last about 20 to 24 months. Unfortunately, duration of orthodontic treatment is the major complaint of patients, especially adults and young adults.
Many attempts have been made to shorten the time for orthodontic tooth movement and overall orthodontic treatment. In 1959, Köle reported on a technique that combined orthodontics with “corticotomy” surgery to increase the rate of orthodontic tooth movement. In 1980, Davidovitch et al. studied how the rate of tooth movement and periodontal cyclic nucleotide levels could be increased by combined force and electrical currents. In 1998, Liou and Huang introduced the technique of distraction of the periodontal ligament for rapid tooth movement.
In 1999, İşeri and Kişnişci introduced a technique called dentoalveolar distraction (DAD), which achieves rapid tooth movement by using the principles of distraction osteogenesis. This chapter presents the associated biological principles, a detailed description of the DAD technique, the data regarding the effects of DAD on the dentofacial structures, and case reports.
BIOLOGICAL PRINCIPLES OF DISTRACTION OSTEOGENESIS
Distraction osteogenesis (DO) is a biological process involving new bone formation between the surfaces of bone segments that are gradually separated by incremental traction. The traction generates tension that stimulates bone formation parallel to the vector of distraction. Specifically, this process is initiated when distraction forces are applied to the callus tissues connecting the divided bone segments and continues as long as these tissues are stretched. Do begins with the development of a reparative callus. The callus is placed under tension by stretching, which generates new bone. DO consists of the following four sequential periods:
- 1.
Osteotomy (or “corticotomy”) means to fracture the bone into two segments. It should be vertical to the direction of distraction.
- 2.
Latency is the period from bone division to the onset of traction (usually 5-7 days) and is the time required for callus formation.
- 3.
Distraction is the period when gradual traction is applied and new bone, or distraction regenerate, is formed. DO has the benefit of simultaneously increasing bone length and the volume of surrounding soft tissues.
- 4.
Consolidation is the period that allows healing and maturation and corticalization of the regenerate after traction forces are discontinued.
In 1988, Ilizarov introduced two biological principles of distraction osteogenesis, known as the Ilizarov effects: (1) the tension stress effect on the genesis and growth of tissues and (2) the influence of blood supply and loading on the shape of bones and joints.
The first Ilizarov principle postulates that gradual traction creates stress that can stimulate and maintain regeneration of living tissues. The newly formed bone rapidly remodels to conform to the bone’s natural structure.
The second Ilizarov principle theorizes that the shape and mass of bones and joints depend on an interaction between mechanical loading and blood supply. Blood supply and mechanical loading have a significant influence on the shape and mass of the resulting bone. If the blood supply is inadequate to support normal and increased mechanical loading, the bone cannot respond favorably, leading to degenerative changes. In contrast, if blood supply is adequate to support increased mechanical loading, the bone will demonstrate compensatory hypertropic changes.
The principles of DO are as follows:
- 1.
Preservation of osteogenic tissues. This is necessary during osteotomy, and periosteum, bone marrow, and the nutrient artery are equally important for new bone formation.
- 2.
Direction of distraction. The regenerate within distraction gap was always formed along the axis of applied traction.
- 3.
Rate and rhythm. Successful distraction depends on the rate and rhythm of the applied distraction force. Optimal rate of distraction is 1 mm per day. More frequent rhythms of distraction lead to more favorable regenerate formation and cause less soft tissue problems. If the rate of distraction is less than 0.5 mm per day, the bone may consolidate prematurely. If the rate of distraction is more than 1.5 mm per day, local ischemia in the interzone and delayed ossification or pseudoarthrosis may result.
Distraction osteogenesis was used as early as 1905 by Codivilla and later popularized by the clinical and research studies of Ilizarov in Russia. DO has been used mainly in the field of orthopedics. In fact, Ilizarov’s concept of long-bone elongation by DO and its application to the craniofacial skeleton opened a new chapter in the treatment of craniofacial anomalies and various malocclusions.
The first report demonstrating the application of Ilizarov’s principles to the dog mandible was published by Snyder et al. in 1973. In this experimental study, the device was activated at a rate of 1 mm per day for 14 days after a 7-day latency period. Reestablishment of the mandibular cortex and medullar canal across the distraction gap was noted after 6 weeks of fixation. In 1977, Michieli and Miotti demonstrated the feasibility of intraoral mandibular lengthening by using Ilizarov’s principles and distraction protocol without damage to the mandible. Lengthening of the mandibular body in two dogs was achieved with a technique that involved osteotomies and the use of an experimental orthodontic appliance without any damage to the mandibular nerve and no conspicuous alterations of the nerve fibers.
Therefore the DO technique is proposed for use in correction of large discrepancies in length in patients with excessive mandibular retrusion. Guerrero (1990) and McCarthy et al. (1992) used DO in the human mandible. In 1999, dentoalveolar distraction (DAD) for rapid tooth movement was described and used by Iseri et al. Since then, DO has been applied to various bones of the craniofacial skeleton.
RAPID TOOTH MOVEMENT BY DENTOALVEOLAR DISTRACTION OSTEOGENESIS
Appliance Design
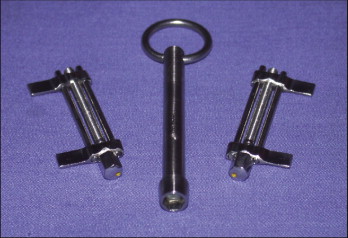
A custom-made, rigid, tooth-borne, intraoral distraction device was designed and used in the DAD patients ( Fig. 25-1 ). The device was made of stainless steel with one distraction screw, two guidance bars, and a special apparatus to activate the distractor by turning the screw clockwise.
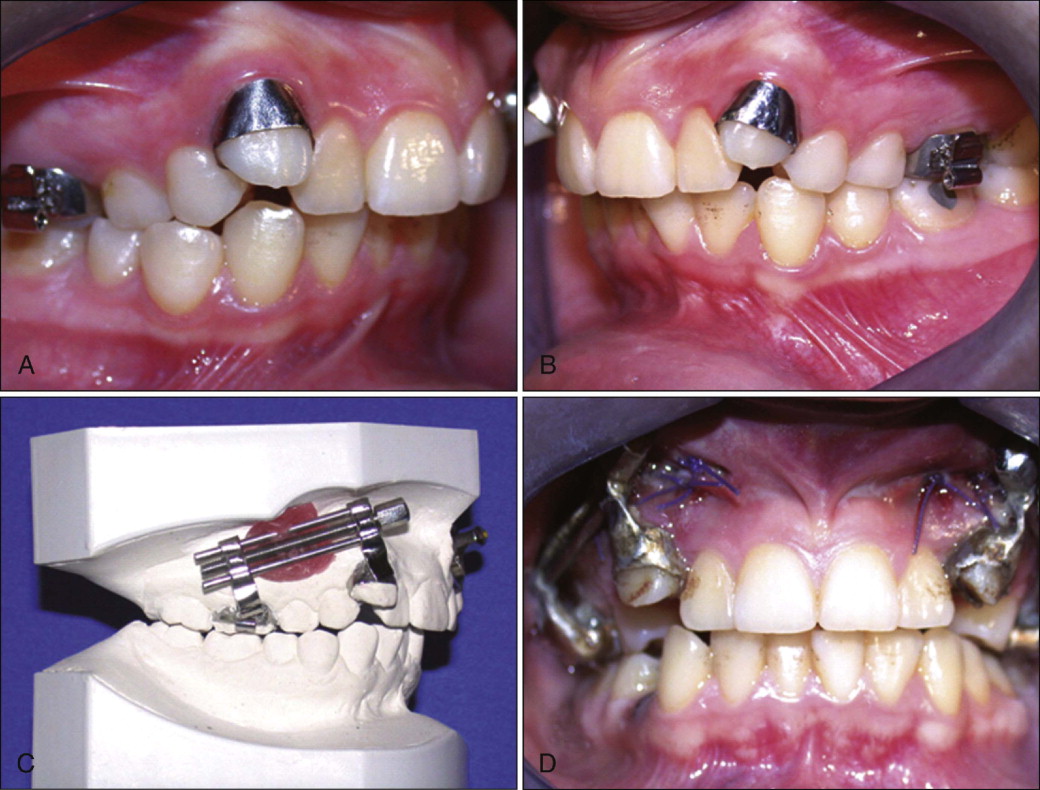
The canines and the first molars were banded with .06 × 1.80–inch (.15 × 4.55–mm) band material, and an impression was made with the bands placed on the teeth ( Fig. 25-2, A and B ). The distractor was then soldered to the canine and first molar bands on the dental cast. The buccal location and angulation of the distractor is adjusted according to the position of the canine ( Fig. 25-2, C ). To minimize tipping, the distractor was positioned as high as possible buccally ( Fig. 25-2, D ).
Surgical Technique
Surgery was performed on an outpatient basis, with the patient under local anesthesia, sometimes supplemented with nitrous oxide sedation. A horizontal mucosal incision 2 to 2.5 cm in length was made parallel to the gingival margin of the canine and premolar beyond the depth of the vestibule ( Fig. 25-3 ).
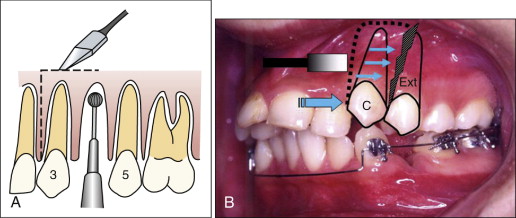
On the medial aspect of the canine tooth to be distracted posteriorly, multiple cortical holes were made on the alveolar bone between the canine and the lateral incisor with a small, round carbide bur ( Fig. 25-4, A and B ). The same procedure was done on the distal aspect of the canine close to the extraction area. Subsequently, the holes around the canine root were connected by a thin, tapered fissure bur ( Fig. 25-4, C ).
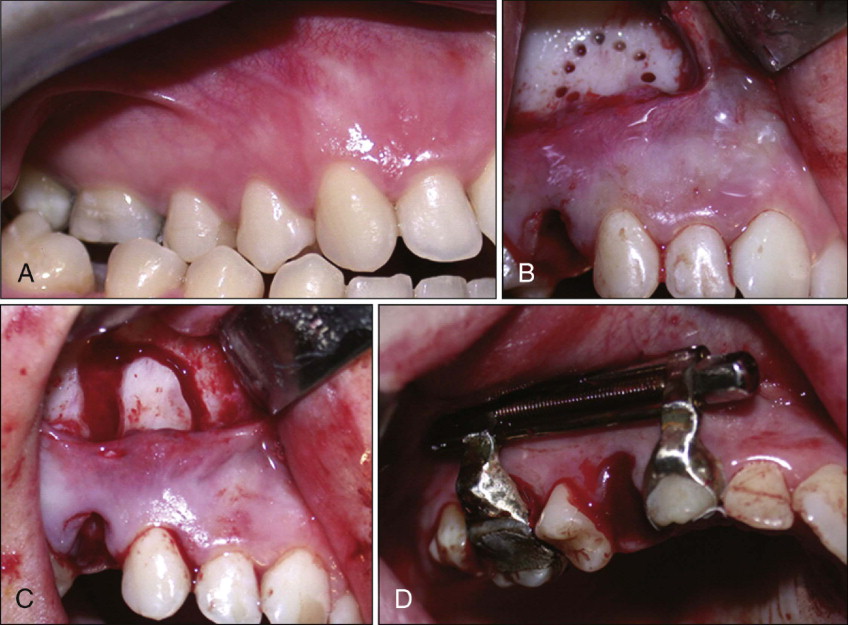
The osteotomy curved apically at a distance of 3-5 mm from the apex. The fine osteotomes were then advanced in the coronal direction. The first premolar was extracted at this stage, and the buccal bone was removed between the outlined bone cut at the distal canine region anteriorly and the second premolar posteriorly by using a large, round bur. Larger osteotomes of appropriate sizes were then used to fully mobilize the alveolar segment, including the canine, by fracturing the spongy bone around its root of the lingual or palatal cortex (see Fig. 25-3 ). The buccal and apical bone through the extraction socket and bony interferences at the buccal aspect that might be encountered during the distraction process were eliminated or smoothed between the canine and the second premolar, preserving the palatal or lingual cortical shelves. Although the palatal shelf was preserved, apical bone near the sinus wall was removed, leaving the sinus membrane intact to avoid interferences during the active distraction process. ( Fig. 25-4, C ). Then, osteotomes along the anterior aspect of the canine were used to split the surrounding bone around its root from the palatal or lingual cortex and neighboring teeth. The transport dentoalveolar segment that included the canine also included the buccal and palatal cortex and the underlying spongy bone that envelopes the canine root, leaving an intact lingual or palatal cortical plate and the bone around the apex of the canine (see Fig. 25-4, C ).
Finally, the DAD device was cemented on the canine and the first molar ( Fig. 25-4, D ). To ensure that the transport segment was fully mobilized, the alveolar segment carrying the canine had been fully mobilized intraoperatively, and the device was activated several millimeters and set back to its original position. The incision was closed with absorbable sutures, and an antibiotic and a nonsteroidal antiinflammatory drug (NSAID) were prescribed for 5 days.
The surgical procedure lasted approximately 30 minutes for each canine. The patients were instructed to discontinue tooth brushing to avoid trauma around the surgical site for 3 days. A 0.2% chlorhexidine gluconate (Klorhex, Drogsan, Ankara, Turkey) rinse was prescribed twice a day during the distraction period.
Distraction Protocol
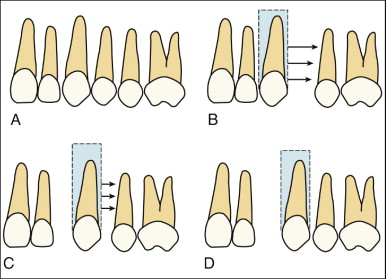
Distraction was initiated within 3 days after surgery. The distractor was activated twice daily, in the morning and in the evening, for a total of about 0.8 mm per day. DAD was based on movement of the alveolar bone as a “transport disk,” which included the canine tooth ( Fig. 25-5 ). This type of distraction is termed as a modification of bifocal osteosynthesis and consists of gradual movement of a vascularized bony segment (transport disk) previously separated from the residual bone segment ( Fig. 25-6 ). New bone is formed during movement of the transport disk in the distraction site with simultaneous closing of the bony defect. In the authors’ cases the alveolar bone was included with the canine.
Dentoalveolar distraction was discontinued when the canine had moved posteriorly into the desired position or came into contact with the second premolar, if necessary. The DAD device (distractor) was then removed, and fixed-appliance orthodontic treatment was immediately initiated by the leveling of both dental arches particularly to benefit from the uncalcified distraction chamber to resolve anterior crowding and also to achieve incisor retraction if necessary. Ligatures were placed under the archwire between the distracted canine and the first molar and kept at least 3 months after the DAD procedure to avoid mesial movement of the canine.
All patients followed a program of meticulous oral hygiene, initiated before and after the DAD procedure and reinforced monthly during fixed-appliance orthodontic therapy, together with professional tooth cleaning.
Orthodontic Tooth Movement
Orthodontic tooth movement is a process in which the application of a force induces bone resorption on the pressure side and bone apposition on the tension side. Thus, conventional tooth movement results from biological cascades of resorption and apposition caused by the mechanical forces. The term physiological tooth movement primarily refers to the slight tipping of the tooth in its socket and secondarily to the changes in tooth position that occur during and after tooth eruption.
Basically, no significant difference exists between the tissue reactions observed in physiological tooth movement and those in orthodontic tooth movement. However, because the teeth are moved more rapidly during treatment, the tissue changes elicited by orthodontic forces are more marked and extensive. Classically, the typical rate of orthodontic tooth movement depends on magnitude and duration of force applied, number and shape of roots, quality of bony trabeculae, individual response, and patient compliance. Presumably, application of force will result in hyalinization from both anatomical and mechanical factors.
The hyalinization period usually lasts 2 to 3 weeks. The rate of biological tooth movement with optimum mechanical force is about 1.0 to 1.5 mm in 4 to 5 weeks. Therefore, in maximum anchorage premolar extraction cases, the canine distalization phase usually takes about 6 to 9 months, with an average overall treatment time of 2 years.
Rapid Tooth Movement
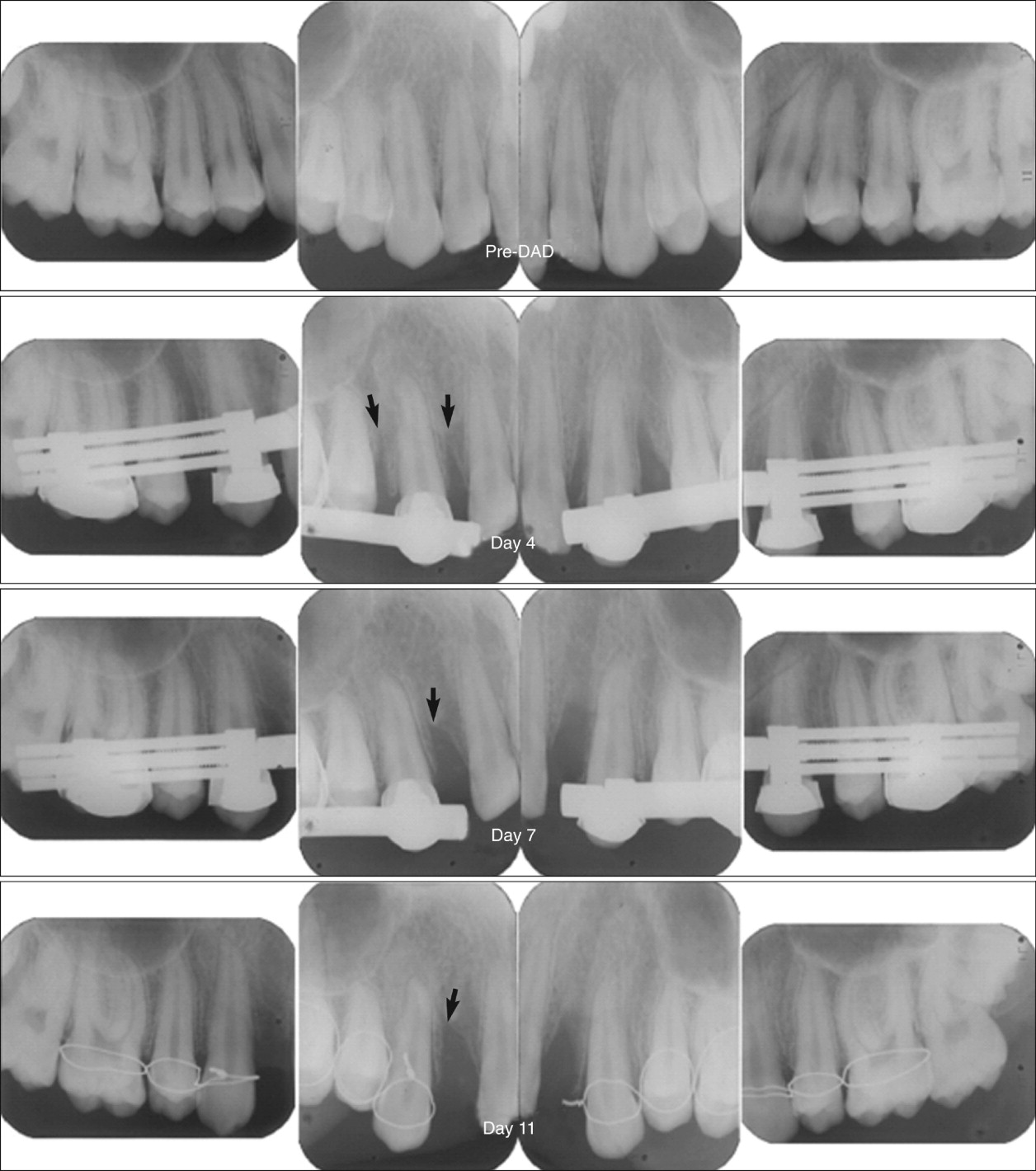
Rapid tooth movement using DO principles is done to shorten the duration of orthodontic treatment. In 2005, İşeri et al. published the duration of canine retraction and the effects of DAD on the dentofacial structures. The study sample consisted of 20 maxillary canines in 10 growing or adult subjects (mean age, 16.53 years; range, 13.08-25.67 years). The canines were moved rapidly into the sockets of the extracted first premolars in compliance with DO principles. The distraction procedure was completed in 8 to 14 days, with a screw-turning rate of 0.8 mm/day ( Fig. 25-7 ). Full retractions of the canines were achieved in 10.05 (±2.01) days ( Table 25-1 ). This was the most rapid orthodontic tooth movement demonstrated compared with previous studies. The distal displacement of the canines was mainly a combination of tipping and translation, with a mean change in canine inclination of 13.15 (±4.65) degrees at the end of the distraction period.

| Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Age, start of distraction (years) | 16.53 | 3.76 | 13.08 | 25.67 |
| Duration of distraction (days) | 10.05 | 2.01 | 8.0 | 14 |
| Rate of screw turning | 0.8 mm/day |
Posterior Anchorage Maintenance
No posterior anchorage loss was observed in any of the DAD cases. In 2005, İşeri et al. reported the mean sagittal and vertical anchorage loss in molar teeth as 0.19 ± 0.31 mm and 0.51 ± 0.93 mm, respectively, during 10 days of rapid distraction of the canines, which was statistically insignificant ( Table 25-2 ).
| Start of Distraction (mean ± SD) | End of Distraction (mean ± SD) | Difference (T Test) (mean ± SD) | |
|---|---|---|---|
| Maxillary Measurements (degrees) | |||
| s n ss | 77.58 ± 4.08 | 77.60 ± 4.11 | 0.05 ± 0.54 |
| NSL/NL | 8.90 ± 3.11 | 9.38 ± 2.45 | 0.49 ± 1.28 |
| Mandibular Measurements (degrees) | |||
| s n sm | 73.57 ± 2.31 | 73.29 ± 2.41 | −0.29 ± 0.63 |
| NSL/ML | 37.94 ± 5.84 | 38.61 ± 5.91 | 0.67 ± 0.80 * |
| Maxillomandibular Measurements | |||
| ss n sm° | 4.10 ± 2.43 | 4.65 ± 2.73 | 0.54 ± 0.97 |
| n me (mm) | 127.00 ± 8.12 | 128.00 ± 8.15 | 0.99 ± 0.57 † |
| Overbite (mm) | 3.19 ± 2.06 | 2.71 ± 1.64 | −0.48 ± 1.20 |
| Overjet (mm) | 5.83 ± 4.16 | 5.50 ± 4.08 | −0.34 ± 0.44 * |
| Dentoalveolar Measurements | |||
| NSL/can inc (degrees) | 93.85 ± 9.82 | 84.20 ± 5.92 | 13.15 ± 4.65 † |
| NSL-is (mm) | 84.39 ± 3.86 | 84.68 ± 4.08 | 0.29 ± 0.62 |
| NSL-ms (mm) | 72.63 ± 3.62 | 73.14 ± 3.77 | 0.51 ± 0.93 |
| NSLv-is (mm) | 101.31 ± 5.40 | 101.31 ± 5.41 | −0.01 ± 1.01 |
| NSLv-ms (mm) | 63.01 ± 7.93 | 62.82 ± 7.91 | 0.19 ± 0.31 |
During orthodontic tooth movement, hyalinized tissue neighboring the tooth on the movement side must be undermined with indirect resorption. This period usually lasts 2 or 3 weeks; again, rapid canine retraction with DAD was achieved in 8 to 14 days, a short period for molars to move mesially (see Figs. 25-6 and 25-7 ).
Root Resorption
Periapical radiographs of the canines and first molars and panoramic films were taken at the start and end of the distraction procedure to evaluate root structures. Root resorption scores were detected according to the scale modified from Sharpe et al., as follows:
- •
S0 = No apical root resorption
- •
S1 = Widening of periodontal ligament (PDL) space at the root apex
- •
S2 = Moderate blunting of the root apex up to one third of the root length
- •
S3 = Severe blunting of the root apex beyond one third of the root length
No clinical or radiographic evidence of complications (e.g., root fracture, root resorption, ankylosis, soft tissue dehiscence) was observed in the DAD patients ( Fig. 25-8 ).

Tooth Vitality
Pulp vitality was evaluated and recorded with an electronic digital pulp tester and a thermal pulp tester. All teeth subjected to pulp vitality tests (canines, incisors, second premolars, first molars) were cleaned and tested on the buccal surfaces.
Before the start of treatment, pulp vitality was tested with an electronic pulp tester. All teeth reacted positively, except for a right maxillary central incisor in a patient with previous root canal therapy. At the end of the DAD procedure and during the fixed-appliance orthodontic treatment, no reliable reactions to the pulp test were achieved in the study subjects. However, all teeth reacted positively at the 6-month evaluation after treatment.
Periodontal Status
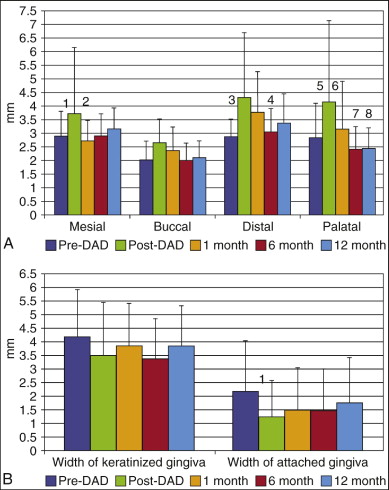
In 2005, Gürgan et al. evaluated the alterations that occurred in the gingival dimensions of canine teeth after DAD during a 12-month follow-up. Before surgery (pre-DAD), immediately after removal of the device (post-DAD), and at 1, 6, and 12 months post-DAD, the plaque index (PI), gingival index (GI), pocket depth (PD), and width of keratinized gingiva were recorded and the width of attached gingiva was calculated ( Fig. 25-9 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


