Armamentarium
|
History of the Procedure
The treatment of mandibular fractures has a long and rich history and can be traced all the way back to Hippocrates. By immobilizing the fractured segment, allowing him to wire adjacent teeth together, Hippocrates initiated the key principles in treating such fractures. Since that time, surgeons have established the importance of restoring appropriate occlusion and maintaining proper muscular balance. Although the techniques now appear crude and antiquated, it is easy to understand the thinking and rationale behind them. Variations of bandages, appliances, splints, and wiring have been used to stabilize the jaws to ensure proper healing and restoration of function. Both bandages and external appliances appeared to be promising in the treatment of mandibular fractures; however, they both produced undesirable posterior directional forces, which could prove deleterious in treating angle and ramus fractures. Splints were developed in the nineteenth century for both the maxilla and the mandible, and they provided stable intermaxillary fixation. Gilmer popularized the use of wires, as he demonstrated excellent intermaxillary fixation through the wiring of arch bars. With improved plating systems used to fixate mobile bony segments, only further refinement and more sophisticated technology were needed to produce the techniques seen today.
History of the Procedure
The treatment of mandibular fractures has a long and rich history and can be traced all the way back to Hippocrates. By immobilizing the fractured segment, allowing him to wire adjacent teeth together, Hippocrates initiated the key principles in treating such fractures. Since that time, surgeons have established the importance of restoring appropriate occlusion and maintaining proper muscular balance. Although the techniques now appear crude and antiquated, it is easy to understand the thinking and rationale behind them. Variations of bandages, appliances, splints, and wiring have been used to stabilize the jaws to ensure proper healing and restoration of function. Both bandages and external appliances appeared to be promising in the treatment of mandibular fractures; however, they both produced undesirable posterior directional forces, which could prove deleterious in treating angle and ramus fractures. Splints were developed in the nineteenth century for both the maxilla and the mandible, and they provided stable intermaxillary fixation. Gilmer popularized the use of wires, as he demonstrated excellent intermaxillary fixation through the wiring of arch bars. With improved plating systems used to fixate mobile bony segments, only further refinement and more sophisticated technology were needed to produce the techniques seen today.
Indications for the Use of the Procedure
Any fracture of the mandible must be properly evaluated and thoroughly assessed, both clinically and radiographically. In fact, radiographic evaluation is of primary importance and the panoramic radiograph is one of the most valuable tools available, especially in ramus and angle fractures. However, a complete mandible film series should be ordered, and the included lateral oblique view can be used to also evaluate the ramus region, whereas the anteroposterior (AP) skull view is important for evaluating potential angle fractures. Nowadays, computed tomography (CT) scans have also become ubiquitous, and these allow for a more detailed view of mandible fractures as well as other concomitant facial injuries. Additionally, CT of the neck should be used to rule out more severe injuries such as cervical spine fractures, which can occur nearly 10% of the time. These injuries, if not identified promptly, can lead to severe neurologic consequences, as C1 and C2 are most commonly involved.
Mandibular angle and ramus fractures constitute less than half of the total number of mandibular fractures at 30% (25% for angle, 4% for ramus). Although ramus fractures remain relatively rare, angle fractures are the third most common and, as such, deserve greater attention. The cross-sectional area of the angle is relatively thin, and coupled with the presence of impacted third molars it is a commonly fractured site. Statistical and literature reviews show that the majority of mandibular fractures occur in accidental or trauma-related incidents. However, when assault cases are further evaluated, it is found that angle fractures constitute a disproportionately high percentage. The general classification of mandibular fractures is comprehensive and discussed in chapters elsewhere; however, those that apply to these particular fracture patterns will be addressed.
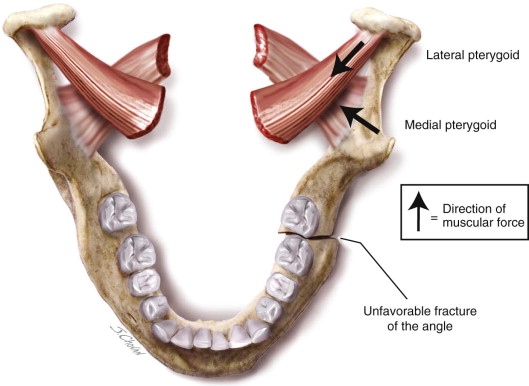
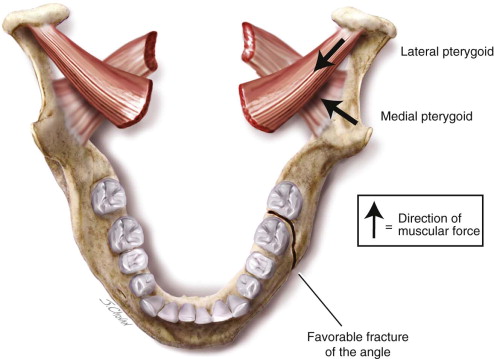
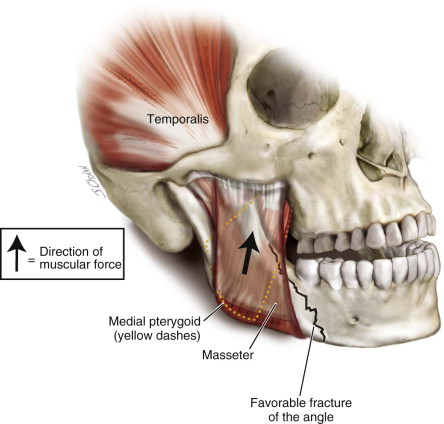
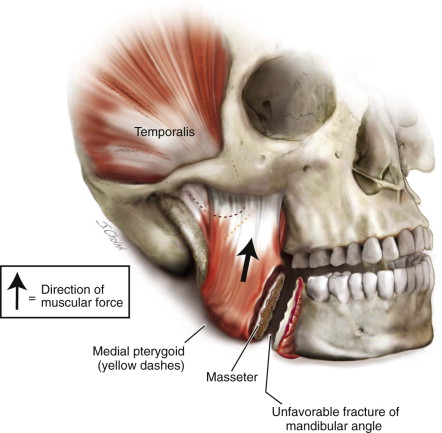
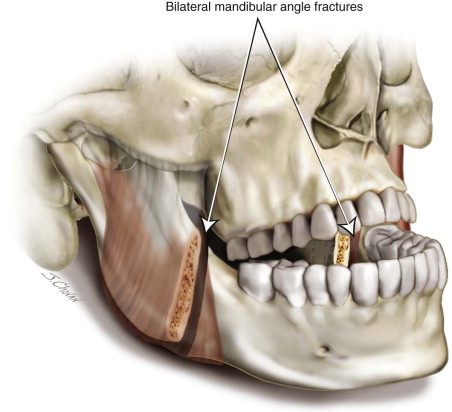
Angle fractures often occur in conjunction with other mandibular fractures, but the muscular attachments often dictate how the segments move in relation to one another. Angle fractures are classified according to their favorability and the direction of muscular force: vertically favorable or unfavorable and horizontally favorable or unfavorable ( Figures 66-1 through 66-4 ). Favorable fractures tend to move the fragments toward each other, whereas unfavorable fractures tend to pull the segments apart ( Figures 66-1 and 66-4 ). The masseter, temporalis, and medial pterygoid all play a role in displacement of fractured segments. Fractures that are unfavorable will lead to displacement of the proximal segment upward and medially, while being impacted in the opposite direction during favorable fractures ( Figures 66-2 and 66-3 ). Due to the severity of forces that occur during a bilateral angle fracture, the patient may suffer from an obvious open bite ( Figure 66-5 ). Ramus fractures are typically classified as favorable due to the elevating forces of the muscles, whereas angle fractures are horizontally unfavorable due to the pull of the same muscles. This favorability of ramus fractures allows for treatment with maxillomandibular fixation (MMF). However, some studies have demonstrated that open reduction and internal fixation (ORIF) of ramus fractures provide adequate functional and anatomic reduction.
Limitations and Contraindications
Once the patient’s history has been taken and physical exam completed, the clinician should decide which diagnostic imaging method is most appropriate for visualizing the fracture. Although the standard set includes a panoramic radiograph and a CT scan, both do have their limitations. Nevertheless, the clinician should supplement their radiologic findings with their clinical findings.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


