Chapter 48 Genioglossus advancement in sleep apnea surgery
Obstructive sleep apnea syndrome is associated with airway obstruction due to a decrease in upper airway muscle tone during sleep. Because the genioglossus muscle is a major pharyngeal dilator, it has long been suggested to play a major role in nocturnal airway obstruction. Genioglossus advancement is a surgical procedure which places the genioglossus muscle under tension, thus restricting the collapse of the tongue into the airway during sleep-induced hypotonia. This chapter describes my technique.
1 INTRODUCTION
Hypopharyngeal obstruction is a major contributing factor in obstructive sleep apnea (OSA). Hypopharyngeal obstruction stems from the prominence or relaxation of the base of the tongue, lateral pharyngeal wall collapse, and occasionally involves the aryepiglottic folds or epiglottis.1–3 Because the genioglossus muscle is a major pharyngeal dilator, it has long been suggested to play a major role in nocturnal airway obstruction.4,5 Genioglossus advancement is a surgical procedure designed to place the genioglossus muscle under tension, thus restricting the collapse of the tongue into the airway during sleep-induced hypotonia. Multiple studies have demonstrated that genioglossus advancement combined with uvulopalatopharyngoplasty achieves improvement of OSA.6–8 Several designs of the osteotomy during genioglossus advancement have been described, with each one aimed at minimizing the surgical morbidity while improving the incorporation and the advancement of the genioglossus muscle.6,9–11
3 SURGICAL TECHNIQUE
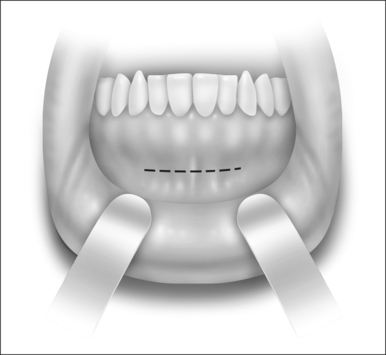
The procedure is performed under general anesthesia with oroendotracheal intubation. Local anesthetic injection (10 milliliters of 2% lidocaine with epinephrine) is administered at the anterior mandibular vestibule. The procedure begins with a mucosal incision approximately 10 mm below the mucogingival junction (Fig. 48.1). A subperiosteal dissection is performed to expose the mandibular symphysis. Exposure and identification of the mental nerves are unnecessary as the mental foramen is lateral to the surgical site. The genial tubercle and genioglossus muscle can be estimated by finger palpation in the floor of the mouth and with the aid of the lateral cephalometric and panoramic radiographs. A rectangular osteotomy encompassing the estimated location of the genial tubercle is performed under copious irrigation (Fig. 48.2). It is recommended that the superior horizontal bone cut be at least 5 mm below the mandibular root apices to decrease the likelihood of tooth paresthesia. The inferior horizontal bone cut should be designed to preserve approximately 10 mm of the inferior border of the mandible to reduce the risk of a pathologic mandibular fracture. If there is insufficient mandibular symphyseal height, this procedure should not be performed as the risk of pathologic mandibular fracture or tooth root injury is increased. Due to the elongated canine tooth roots that are often present, the vertical bone cuts are made just medial to the canine tooth to avoid root injury. It is crucial to follow parallelism of the osteotomies to facilitate the ease of releasing the rectangular bone flap. Prior to completing the osteotomy, a titanium screw is placed in the outer cortex to control and manipulate the bone flap. At the completion of the osteotomy, the bone flap is released from the surrounding bone and is advanced and rotated 60° to prevent retraction back into the floor of the mouth. The outer cortex and marrow are removed and the inner cortex is rigidly fixed with a lag screw (Fig. 48.3).
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


