Armamentarium
|
History of the Procedure
The first recorded approaches for surgical management of craniosynostosis were documented in 1890 and 1892 by Lannelogue and Lane, respectively. Their papers described the classical elements of what we understand today to be a strip craniectomy. In this procedure, the affected fused suture was excised in an attempt to limit brain compression or intracranial hypertension. As time progressed, modifications of the strip craniectomy were made in an attempt to also improve residual skull shape after surgery with the assistance of brain growth. Then, as now, improvements to the skull shape were limited.
Tessier accomplished a major breakthrough in 1967 when he described the transcranial approach to the upper orbits through the skull base. This revolutionized thinking about craniofacial surgery and formed the technical underpinning of many of the approaches in modern use today, especially in patients with craniofacial dysostosis. Rougerie expanded on this approach and included remodeling of the anterior cranial vault simultaneously. Hoffman and Mohr described the lateral canthal advancement procedure in 1976, and in 1977 Whitaker and colleagues proposed more extensive anterior cranial vault remodeling with orbital advancement. In 1979, Marchac and Renier described the floating forehead technique, in which the bandeau segment was loosely attached to the remaining orbits accompanied by vault reshaping. They argued that the principal advantage of this technique was that it allowed brain growth to push further forward the upper face in a symmetric fashion. Unfortunately, this advantage failed to materialize for most patients postoperatively. Most recently, the incorporation of resorbable fixation as a method of providing stability to the orbits and forehead to limit relapse has been widely successful and has eliminated the risk of transcranial screw migration in infants. Gaining popularity as a method of treatment for craniosynostosis is the limited access/endoscopic technique, which, ironically, is essentially an extended strip craniectomy.
History of the Procedure
The first recorded approaches for surgical management of craniosynostosis were documented in 1890 and 1892 by Lannelogue and Lane, respectively. Their papers described the classical elements of what we understand today to be a strip craniectomy. In this procedure, the affected fused suture was excised in an attempt to limit brain compression or intracranial hypertension. As time progressed, modifications of the strip craniectomy were made in an attempt to also improve residual skull shape after surgery with the assistance of brain growth. Then, as now, improvements to the skull shape were limited.
Tessier accomplished a major breakthrough in 1967 when he described the transcranial approach to the upper orbits through the skull base. This revolutionized thinking about craniofacial surgery and formed the technical underpinning of many of the approaches in modern use today, especially in patients with craniofacial dysostosis. Rougerie expanded on this approach and included remodeling of the anterior cranial vault simultaneously. Hoffman and Mohr described the lateral canthal advancement procedure in 1976, and in 1977 Whitaker and colleagues proposed more extensive anterior cranial vault remodeling with orbital advancement. In 1979, Marchac and Renier described the floating forehead technique, in which the bandeau segment was loosely attached to the remaining orbits accompanied by vault reshaping. They argued that the principal advantage of this technique was that it allowed brain growth to push further forward the upper face in a symmetric fashion. Unfortunately, this advantage failed to materialize for most patients postoperatively. Most recently, the incorporation of resorbable fixation as a method of providing stability to the orbits and forehead to limit relapse has been widely successful and has eliminated the risk of transcranial screw migration in infants. Gaining popularity as a method of treatment for craniosynostosis is the limited access/endoscopic technique, which, ironically, is essentially an extended strip craniectomy.
Indications for the Use of the Procedure
Craniosynostosis is defined as the premature fusion of one or more of the cranial vault sutures. Virchow first described the sequence of events that adversely affect skull growth in the presence of craniosynostosis. Growth is arrested in a direction perpendicular to the fused suture, whereas there is a compensatory amount of overgrowth at the sutures that remain open (Virchow’s law). This disrupted growth pattern creates a characteristic dysmorphology and a bilateral deformity.
If the rapid brain growth that normally occurs during infancy is to proceed unhindered, the cranial vault and base sutures must remain open and expand during phases of rapid growth, resulting in marginal ossification. In craniosynostosis, premature fusion of the suture causes limited and abnormal skeletal expansion in the presence of continued brain growth. Depending on the number and location of prematurely fused sutures, the growth of the brain may be restricted. In addition, abnormal cranial vault and midfacial morphology occurs as determined by Virchow’s law. If the affected sutures are not surgically released and reshaped to restore a more normal intracranial volume and configuration, decreased cognitive and behavioral function is likely to result.
Elevated intracranial pressure (ICP) is the most serious functional problem associated with premature suture fusion. Untreated craniosynostosis with elevated ICP will cause papilledema and eventual optic nerve atrophy, resulting in partial or complete blindness. If the orbits are shallow (exorbitism) and the eyes are proptotic (exophthalmus), as occurs in the craniofacial dysostosis syndromes, the cornea may be exposed and abrasions or ulcerations may occur. An eyeball extending outside of a shallow orbit is also a risk for trauma. If the orbits are extremely shallow, herniation of the globe itself may occur, necessitating emergency reduction followed by tarsorrhaphies or urgent orbital decompression.
Some forms of craniofacial dysostosis result in a marked degree of orbital hypertelorism, which may compromise visual acuity and restrict binocular vision. Divergent or convergent nonparalytic strabismus or exotropia occurs frequently and should be considered during the diagnostic evaluation. This may be the result of congenital anomalies of the extraocular muscles themselves. Paralytic or nonparalytic unilateral or bilateral upper eyelid ptosis also occurs with greater frequency than what is encountered in the general population.
Hydrocephalus affects as many as 10% of patients with a craniofacial dysostosis syndrome. Although the etiology is often not clear, hydrocephalus may be secondary to a generalized cranial base stenosis with constriction of all the cranial base foramina, which impacts the patient’s cerebral venous drainage and cerebrospinal fluid (CSF) flow dynamics.
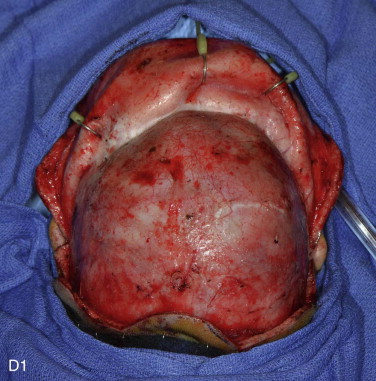
The surgical management of craniosynostosis involves release of the fused suture and dismantling of the fused and dysmorphic skeletal components via craniotomy followed by reconstruction to reassemble those structures into a more normal anatomic position. As a result, the reconstructive approach must address the orbital deformity. Correction generally involves the creation of a fronto-orbital bandeau that is reshaped as part of the overall reconstruction.
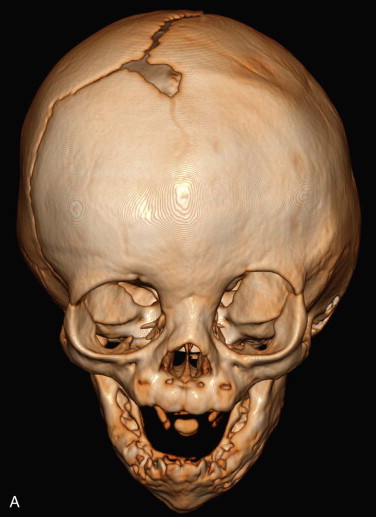
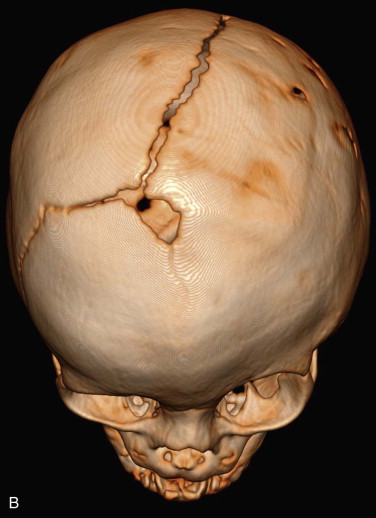
Fronto-orbital advancement with anterior cranial vault reshaping is ideally reserved for the management of patients who have a diagnosis of isolated craniosynostosis or craniofacial dysostosis (syndromic craniosynostosis) involving the metopic, sagittal, unilateral coronal, or bilateral coronal sutures ( Figure 43-1 ). Additionally, it can be utilized as a selected surgical technique in unique skull base pathologies (i.e., craniofacial fibrous dysplasia).




Establishing normal position of the forehead is critical to overall facial symmetry and balance. The forehead may be considered as two separate esthetic components: the supraorbital ridge–lateral orbital rim region and the superior forehead. The supraorbital ridge–lateral orbital rim region includes the glabella and supraorbital rim extending inferiorly down each frontozygomatic suture toward the infraorbital rim and posteriorly along each temporoparietal region. The morphology and position of the supraorbital ridge–lateral orbital rim region is a key element of upper facial esthetics. In a normal forehead, at the level of the frontonasal suture, an angle ranging from 90 degrees to 110 degrees is formed by the supraorbital ridge and the nasal bones when viewed in profile. Additionally, the eyebrows, overlying the supraorbital ridge, should be anterior to the cornea. When the supraorbital ridge is viewed from above, the rim should arc posteriorly to achieve a gentle 90-degree angle at the temporal fossa with a center point of the arc at the level of each frontozygomatic suture. The superior forehead component, about 1.0 to 1.5 cm up from the supraorbital rim, should have a gentle posterior curve of about 60 degrees, leveling out at the coronal suture region when seen in profile.
Technique: Fronto-Orbital Advancement and Anterior Cranial Vault Reshaping
Step 1:
Patient Preparation
General anesthesia is induced with placement of an oral (reinforced) endotracheal tube. The tube is generally secured in the midline.
The anesthetic team carries out placement of venous access (two peripheral venous lines or one central venous line) and an arterial line for intraoperative blood pressure monitoring. A Foley catheter is placed.
Step 2:
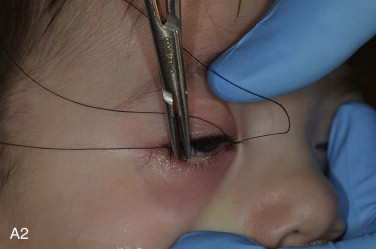
Tarsorrhaphy
Temporary tarsorrhaphy sutures are placed for corneal protection during the surgical procedure. The upper eyelid is gently retracted with a finger and held in place. A 5-0 silk suture on a noncutting (tapered) needle is passed through the gray line (canthal line) of the eyelid. The finger being used to retract the eyelid is kept in place until the needle driver recaptures the needle (this prevents movement of the eyelid, which can cause the needle to injure the cornea). The suture is passed through the lower eyelid in similar fashion, again with the index finger used to hold the position of the eyelid until the needle is recaptured safely.
The operating table is then turned 90 degrees from the anesthesia team, and the patient is positioned with the head in a horseshoe-shaped Mayfield type head holder and padding of all pressure points. During positioning, maintenance of the cervical spine in a neutral position is confirmed ( Figure 43-2, A, B ).







Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


