Armamentarium
|
History of the Procedure
Medical modeling and simulation have been developed over the past 20 years by software engineers partnering with health care professionals to enable the transfer of clinical information to computer-based planning programs. The technologic advances have allowed health care professionals to be more precise, to become better teachers, and to improve the care of the general public. This technology is used not only in oral and maxillofacial surgery, but also in many other specialties, such as neurosurgery and otolaryngology.
In 2003, Gateno et al published two papers on the use of three-dimensional (3D) surgical planning for jaw surgery, in addition to the techniques for creating a composite 3D skull model. In 2007 these same researchers published work on feasibility studies for using computer-assisted surgical simulation systems in the treatment of dentofacial deformitites. In 2013, Hsu et al published the data of three teams in a multicenter study evaluating the accuracy of computer-aided design for corrective jaw surgery and found that the protocols and procedures produced accurate results.
Use of a digital platform for planning and executing skeletal facial movements has quickly become a routine methodology of treatment. However, despite its rapid acceptance, this technology is not a substitute for sound treatment planning that incorporates the surgeon’s understanding of jaw function, long-term stability, and facial aesthetics. All of these factors must still be included in the treatment planning process, regardless of whether the surgeon uses traditional model surgery planning techniques or a digital model surgery platform.
History of the Procedure
Medical modeling and simulation have been developed over the past 20 years by software engineers partnering with health care professionals to enable the transfer of clinical information to computer-based planning programs. The technologic advances have allowed health care professionals to be more precise, to become better teachers, and to improve the care of the general public. This technology is used not only in oral and maxillofacial surgery, but also in many other specialties, such as neurosurgery and otolaryngology.
In 2003, Gateno et al published two papers on the use of three-dimensional (3D) surgical planning for jaw surgery, in addition to the techniques for creating a composite 3D skull model. In 2007 these same researchers published work on feasibility studies for using computer-assisted surgical simulation systems in the treatment of dentofacial deformitites. In 2013, Hsu et al published the data of three teams in a multicenter study evaluating the accuracy of computer-aided design for corrective jaw surgery and found that the protocols and procedures produced accurate results.
Use of a digital platform for planning and executing skeletal facial movements has quickly become a routine methodology of treatment. However, despite its rapid acceptance, this technology is not a substitute for sound treatment planning that incorporates the surgeon’s understanding of jaw function, long-term stability, and facial aesthetics. All of these factors must still be included in the treatment planning process, regardless of whether the surgeon uses traditional model surgery planning techniques or a digital model surgery platform.
Indications for the Use of the Procedure
Computer planning and design are used in oral and maxillofacial surgery to plan osteotomies for orthognathic surgery, distraction surgery, tumor debulking, and resection/reconstructive surgery. Computer planning also is used to create stereolithic models for planning and machine-generated splints to use in the operating room to guide the surgeon to the digitally planned result. In addition, computer planning is used in stereotactic surgery, for navigation during difficult 3D movement or reconstructive surgery.
Limitations and Contraindications
There are no known contraindications to computer planning. However, financial constraints may be a factor. These financial issues include the purchase of the necessary equipment, including hardware and software, and fees for processing the information and fabrication of the models and splints.
Unless a proper-quality DICOM data set is sent to the modeling company, an accurate model and surgical guides cannot be fabricated. Clinical records also must be excellent to transfer the data and “mount” the case in the computer in natural head position (NHP).
Technique: Registration of Centric Relation (CR) and Digital Face-Bow
Step 1:
Workup with Bite Jig (Fork) and Digital Gyroscope: Bite Registration
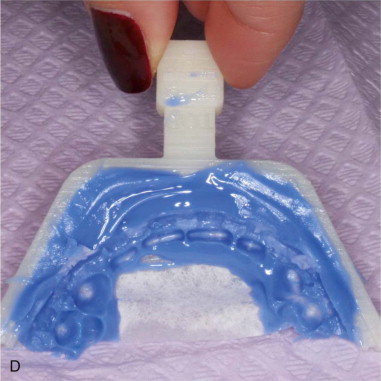
Take the CR bite registration with a stiff material on the bite forks provided by modeling company. Take care to have only the anterior part of the dentition in the bite, from premolars forward. Have the teeth in CR occlusion in the posterior region so as not to rotate the bite open on the scan; otherwise, this will distort the condylar position. Also, the bite material should have minimal distortion ( Figure 28-1, A to G ).









Step 2:
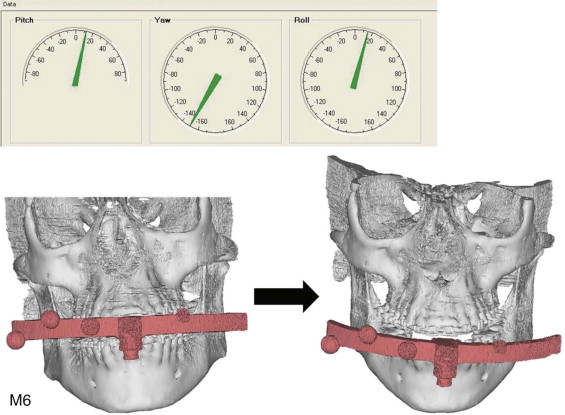
Natural Head Position Registration
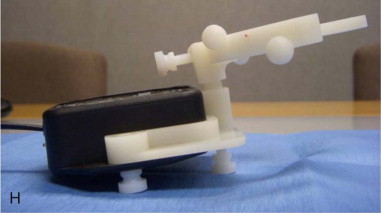
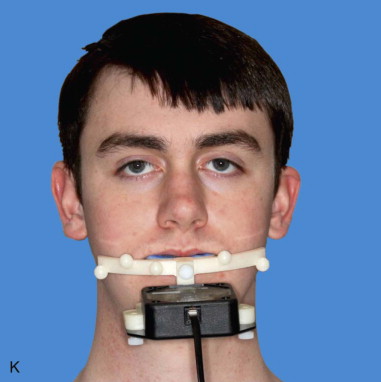
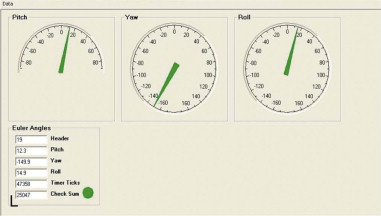
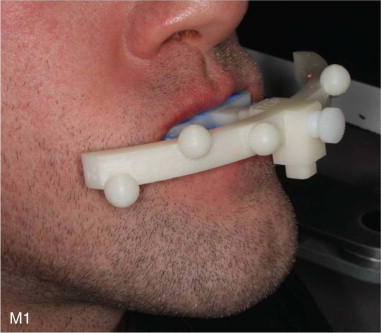
Register the NHP with a digital gyroscope; take three readings and record them. The bite fork is attached to the radiographic fiducial markers of the digital face-bow. The bow is connected to the gyroscope, which is attached to the computer directly by a cord. Euler angles (pitch, roll, and yaw) are recorded three times. The engineers take an average of these three readings to set the head position ( Figure 28-1, H to L ).
Step 3:
CT Scanning
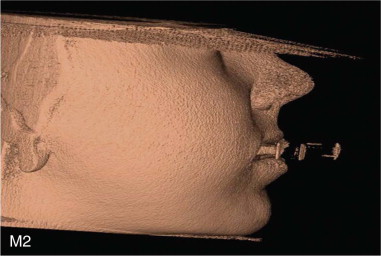
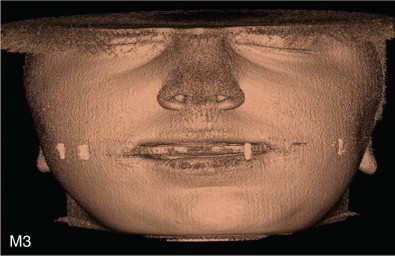
Take a CT scan with the CR bite in the patient’s mouth attached to the fiducial markers of the digital face-bow. Note that the gyroscope is not connected any longer to the bite fork once the registrations are done in Step 2 ( Figure 28-1, M ).
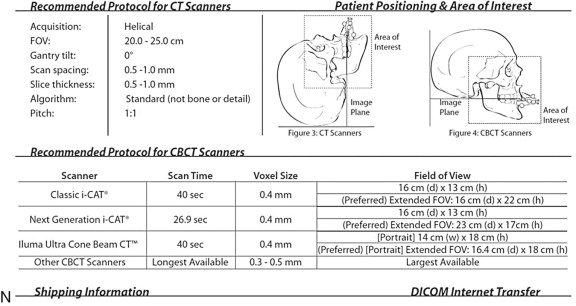
Different CT scan machines require different protocols. These protocols should be investigated ahead of time to ensure adequate digital information capture ( Figure 28-1, N ).
Step 4:
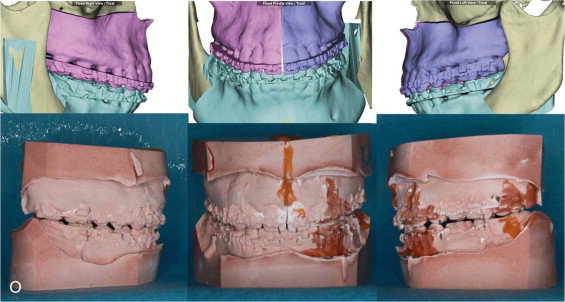
Facial Measurements
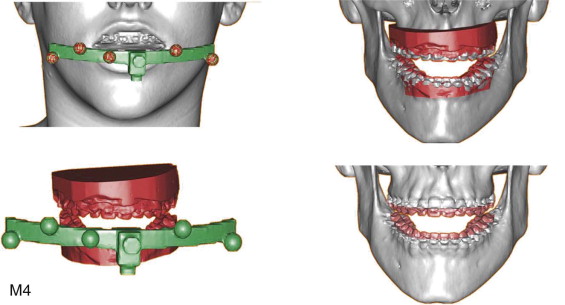
Take facial soft tissue measurements and record them. These are used to make the surgical plan, along with cephalometric analysis, before the computer model surgery session. The engineers also need to see these data to make digital mounting more accurate.
Step 5:
Data Transmission to Engineers
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


