In this article, we report the successful use of miniscrews in a patient with an Angle Class III malocclusion, lateral open bite, midline deviation, and severe crowding. Simultaneously resolving such problems with conventional Class III treatment is difficult. In this case, the treatment procedure was even more challenging because the patient preferred to have lingual brackets on the maxillary teeth. As a result, miniscrews were used to facilitate significant asymmetric tooth movement in the posterior and downward directions; this contributed to the camouflage of the skeletal mandibular protrusion together with complete resolution of the severe crowding and lateral open bite. Analysis of the jaw motion showed that irregularities in chewing movement were also resolved, and a stable occlusion was achieved. Improvements in the facial profile and dental arches remained stable at the 18-month follow-up.
When treating adult Class III patients without orthognathic surgery, various methods have been used, including multi-brackets with Class III elastics, extraction treatment, and multi-loop edgewise therapy. These techniques facilitate acceptable interincisal relationships and stable occlusions; however, most require intraoral or extraoral anchorage to retract the mandibular incisors, and the quality of the treatment result often depends on the patient’s cooperation.
Recently, implant anchorage has been used in a wide variety of adult malocclusions. In particular, miniscrews have been used as temporary anchorage devices because procedures for placement and removal are less invasive than with other implants. Despite their small diameter and short length, miniscrews can achieve stable anchorage for various tooth movements, including intrusion, retraction, and protraction.
In this report, we demonstrate the use of miniscrews in an adult Class III patient with a lateral open bite, severe crowding, and midline deviation who did not wish to undergo an orthognathic surgical procedure. Correcting such a complex situation with conventional Class III treatment is difficult in the best of circumstances. This patient preferred lingual bracket treatment for esthetic reasons. Miniscrew treatment facilitated significant asymmetric tooth movement in the posterior and downward directions; this contributed to the camouflage of the skeletal mandibular protrusion together with complete resolution of the severe crowding and the lateral open bite.
Diagnosis and etiology
A woman, aged 28 years 9 month, came to our hospital in Okayama, Japan, for treatment with the chief complaint of crooked teeth. ( Figs 1 and 2 ). She strongly desired treatment with an invisible appliance. The concave profile was due to a prognathic mandible and lower lip protrusion. Circumoral muscle strain on mouth closure was observed. A lateral open bite with a reduced overjet of 0.5 mm and a shallow overbite of 0.5 mm were observed. Severe crowding was present in both arches (arch-length discrepancies: maxilla, –13 mm; mandible, –10 mm). The maxillary canines were labially displaced, and the left second premolar was completely displaced toward to the palate. The mandibular incisors were inclined to the right side, and both canines were labially positioned. The mandibular right second premolar was absent. The molar relationships were Angle Class III on both sides. The mandibular molars were mesially inclined. The maxillary dental midline was deviated 2 mm toward the left of the facial midline, and the mandibular dental midline was shifted 6 mm to the right compared with the facial midline. The dental radiographs showed no horizontal or vertical bone loss and a normal root length ( Fig 3 ). Based on the left-chewing record (version 1.31, Gnathohexagraph system, Ono Sokki, Kanagawa, Japan), the jaw movement showed a chopping type of jaw movement pattern. The gap between the opening and closing loci of the right-sided condylar movement was observed on a maximum open-close movement record.

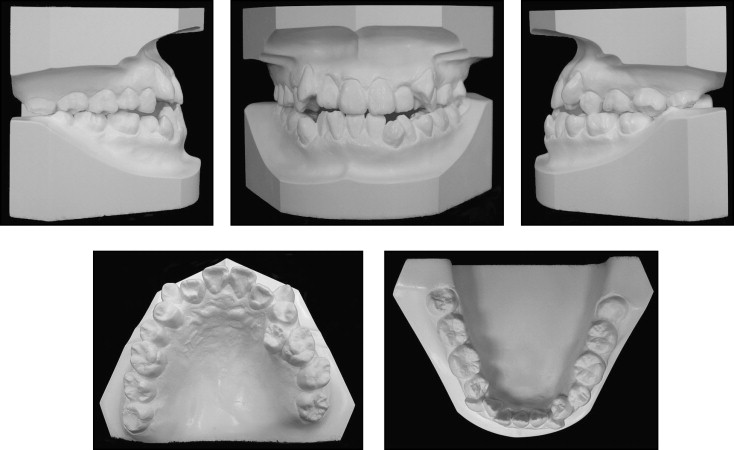
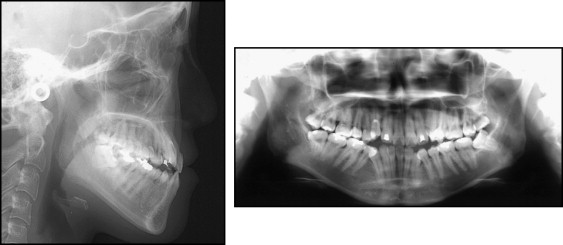
In comparison with the Japanese norm, a skeletal Class III relationship (ANB angle, –3.6°) with maxillary retrusion (SNA angle, 75.2°) was observed ( Table I ). The size of the maxilla was small (Ptm-A/NF, 43.6 mm; Ptm-ANS/NF, 46.2 mm), but the mandibular ramus height and the body length were within the normal ranges (Ar-Me, 108.9 mm; Go-Me, 71.7 mm; Ar-Go, 48.7 mm). The mandibular plane angle was normal (Mp-SN, 39.2°). The maxillary incisor position was almost average (U1/NF, 33.0 mm; U1-SN, 99.8°), but the mandibular incisors were lingually inclined (L1-Mp,m 77.1°), and the interincisal angle was excessive (IIA, 143.8°). The occlusal plane angle was steep (24.3°).
| Mean | SD | Pretreatment | Posttreatment | |
|---|---|---|---|---|
| Angular analysis (°) | ||||
| SNA | 80.8 | 3.61 | 75.2 | 75 |
| SNB | 77.9 | 4.54 | 78.8 | 76.1 |
| ANB | 2.8 | 2.44 | −3.6 | −1.1 |
| Mp-SN | 37.1 | 4.64 | 39.2 | 41.2 |
| Gonial angle | 122.1 | 5.29 | 125.3 | 127.1 |
| U1-SN | 105.9 | 8.79 | 99.8 | 106.2 |
| L1-Mp | 93.4 | 6.77 | 77.1 | 83.1 |
| IIA | 123.6 | 10.64 | 143.8 | 129.6 |
| Occ p | 16.9 | 4.4 | 24.3 | 20.4 |
| Linear analysis (mm) | ||||
| PTM-A/PP | 47.9 | 2.8 | 43.6 | 42.2 |
| PTM-ANS/PP | 52.1 | 3.04 | 46.2 | 45.2 |
| Go-Me | 71.4 | 4.14 | 71.7 | 70 |
| Ar-Go | 47.3 | 3.33 | 48.7 | 48.7 |
| Ar-Me | 106.6 | 5.74 | 108.9 | 106.9 |
| U6/PP | 24.6 | 2 | 23.4 | 25.6 |
| U1/PP | 31 | 2.34 | 33 | 31.1 |
| L6/Mp | 32.9 | 2.5 | 33.8 | 30.6 |
| L1/Mp | 44.2 | 2.68 | 40.2 | 40.1 |
| Overjet | 3.1 | 1.07 | 1.6 | 3.2 |
| Overbite | 3.3 | 1.89 | 1.5 | 1.4 |
Treatment objectives
We diagnosed this patient with an Angle Class III malocclusion, a skeletal Class III jaw-base relationship, lateral open bite, severe maxillary and mandibular crowding, and midline deviation. The treatment objectives were to (1) correct the severe crowding, midline deviation, and lateral open bite; (2) establish an ideal incisor relationship; (3) achieve acceptable occlusion with favorable functional Class I occlusion; and (4) correct the concave facial profile. Because the mandibular molars were significantly inclined mesially, we planned to place miniscrews in the retromolar area to provide skeletal anchorage for their uprighting. Additionally, extraction of 3 premolars and all third molars was required to correct the severe crowding and the midline deviation.
Treatment objectives
We diagnosed this patient with an Angle Class III malocclusion, a skeletal Class III jaw-base relationship, lateral open bite, severe maxillary and mandibular crowding, and midline deviation. The treatment objectives were to (1) correct the severe crowding, midline deviation, and lateral open bite; (2) establish an ideal incisor relationship; (3) achieve acceptable occlusion with favorable functional Class I occlusion; and (4) correct the concave facial profile. Because the mandibular molars were significantly inclined mesially, we planned to place miniscrews in the retromolar area to provide skeletal anchorage for their uprighting. Additionally, extraction of 3 premolars and all third molars was required to correct the severe crowding and the midline deviation.
Treatment alternatives
Two major procedures (with or without orthognathic surgery) were explored to achieve an ideal Class I occlusion. Although maxillary advancement with orthognathic surgery is considered an effective treatment method, the patient did not want to undergo surgery because of social and physiologic reasons, the requirement of prolonged hospitalization, the physical disadvantage of surgical invasion, and her feeling of no dissatisfaction with her facial profile. Therefore, we chose the nonsurgical treatment with premolar extraction using miniscrew anchorage.
Treatment progress
The maxillary first premolars, mandibular left first premolar, and all third molars were extracted before orthodontic treatment. The 0.018-in slot preadjusted edgewise appliances were placed palatally in the maxilla and labially in the mandible, and the leveling of both arches was started. After the leveling of the mandibular arch, except for the right canine and second premolar, 0.016 × 0.022-in stainless steel archwires were positioned, and miniscrews (diameter, 1.3 mm; length, 10 mm; Abso Anchor, Dentos, Taegu, South Korea) were placed in the retromolar area approximately 5 mm distal to the mandibular second molar, as previously reported ( Fig 4 ). Then the mandibular molars were retracted with a nickel-titanium closed-coil spring (200 g) for 12 months. The created spaces were used to correct the crowding and the midline deviation, and improve the inclination of the mandibular incisors. A positive overjet remained throughout the active treatment period ( Fig 5 ). To correct the maxillary midline, we implanted a miniscrew (diameter, 1.5 mm; length, 9 mm; KLS Martin, Umkirch, Germany) in the right buccal area after closure of the extraction space.



