Chapter 3
Understanding Human Error
In recent years the issues of patient safety and healthcare error have become important topics in health policy and healthcare practice in many countries, including the United States, Australia and Great Britain. The extent of the commitment is reflected in some key international publications:
-
In the United States, the Institute of Medicine published To Err is Human: Building a Safer Health System (National Academy of Sciences, 2000). The report is part of a larger project examining the quality of healthcare in America.
-
In Australia, the recommendations of the National Expert Advisory Group on Safety and Quality in Australian Healthcare led to the formation of the Australian Council for Safety and Quality in Healthcare.
-
In the UK, the National Patient Safety Agency was formed in July 2001 following the publication of two reports on patient safety in the NHS An Organisation with a Memory (Department of Health, 2000), and the follow-up document Building a Safer NHS for Patients (Department of Health, 2001).
These initiatives have much in common and reflect the priorities summarised by Baker and Norton (2001), which are to:
-
Improve measurement to increase the detection of adverse events.
-
Provide a reporting system so others can learn from the error.
-
Support healthcare teams and individual practitioners in identifying and preventing adverse events.
-
Encourage the implementation of new tools to mitigate the impact of those events that escape detection.
We must accept that a policy of zero tolerance for errors in general dental practice is unrealistic. Our objective, then, should be to minimise the incidence of error in clinical practice.
All caring clinicians aim for perfection in their work, knowing that it may not be achieved. We also recognise that accidents are inevitable because:
-
All clinicians, regardless of their knowledge, skills and experience, make fallible decisions. There may be ways of moderating this, but we can never eliminate the possibility. Alexander Pope’s maxim “To err is human, to forgive divine” holds true.
-
No matter how well organised and designed your practice systems may be, any system has the potential for failure. James Reason, Professor of Psychology at Manchester University and a world authority on human error, likens this latent potential to resident pathogens in the human body. In the presence of local trigger factors like stress, they are able to overcome the immune system and produce disease. Reason suggests: “As in the case of the human body, no technological system can ever be entirely free of pathogens.”
-
All clinical dental procedures involve an element of risk. The hazards may be understood and we may take steps to protect our patients and ourselves, but our countermeasures cannot be absolute.
There is little training in risk management in the dental undergraduate curriculum; the subject is not perceived as a priority. There are some notable exceptions, however. For example, Michigan State University Kalamazoo Centre for Medical Studies includes an error-in-medicine module. The aim of the module is to teach students to:
-
Understand the scope and gravity of error in healthcare settings.
-
Gain a familiarity with human perceptual limitations and cognitive biases, and learn that they are uncontrollable, yet very predictable.
-
Know theoretical and practical reasons why “blame and train” and “bad apples” approaches fail.
-
Understand the importance of discovering root causes towards proper countermeasures.
-
Become familiar with human-factor engineering and continuous quality improvement techniques that determine root causes and help design countermeasures.
-
Understand that some latent errors and systemic problems are exacerbated by poor design.
This chapter is based on these objectives and draws on the work of Professor James Reason, whose work has been cited in most (if not all) medical publications concerned with error and accident prevention.
The Meaning of Human Error
The term “human error” is a part of our everyday language. When there is an adverse outcome we may attribute it to human error without necessarily understanding the meaning of error or its classification. If risk management is to be effective and we want to prevent the recurrence of errors, we must first understand what we mean by it.
In everyday communication, the words and phrases we use may have a common denotation, but can have different connotations; in the case of human error, however, the term has common connotations but different denotations. The fact is that everyone understands something by it and this leads us to the (false) conclusion that its meaning is well defined and that everyone understands it in the same way. We assume that other people’s understanding is the same as ours.
An editorial in a recent issue of the Journal of Effective Clinical Practice put it more bluntly: “To most of us, an error is a screw-up. The word connotes unambiguous culpability: Someone is to blame.”
It comes down to semantics. The term “human error” has at least three different denotations (Fig 3-1). The examples are situations that many clinicians may be familiar with – all attributed to human error, but quite different in their focus. In terms of clinical practice, we can also classify errors in a different way (see Table 3-1).
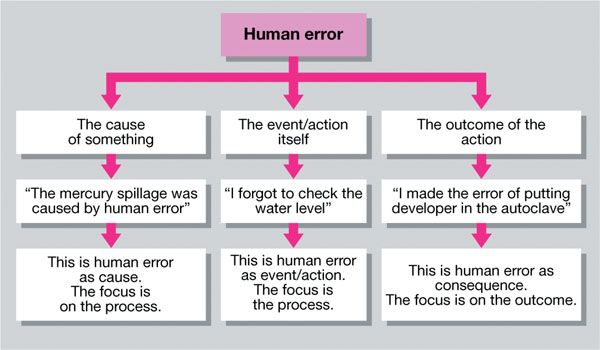
Fig 3-1 The meaning of human error.
| Types of Errors | Clinical Examples | |
| Diagnostic | Error in diagnosis. Delay in diagnosis. Ineffective or inappropriate special tests. Failure to act on results of special tests. Failure to refer when diagnosis is uncertain. |
Failure to detect caries. Failure to diagnose chronic periodontal disease. Diagnosis based on poor-quality radiograph. Failure to act on radiographic evidence. No second opinion sought. |
| Treatment | Error in performing the clinical procedure. Delay in treatment resulting in progression of condition. Ineffective treatment. |
Extraction of wrong tooth. Caries progression requiring need for endodontic therapy. No change in pocket depth after periodontal treatment. |
| Preventive | Failure to provide prophylactic treatment. Failure to prevent medical complications. |
Lack of ongoing perio-dontal therapy in high-risk patient. Failure to provide prophylactic antibiotic cover for patient with relevant medical history. |
| Other | Failure of communication. Equipment failure. System failure. | Mismatch in expectations between dentist and patient. Using faulty equipment. Referral letter not sent. |
To understand what we mean by the term is central to how we manage situations which we attribute to “human error” and, more importantly, what we do to prevent their recurrence.
Primary Care International Study of Medical Errors
The Primary Care International Study of Medical Errors (PCISME) – 2001 was the first international study of medical errors in general medical practice and involved six countries with similar primary healthcare standards. The aim was to classify the types of errors recognised by healthcare providers and to develop an international taxonomy of the errors reported.
In the PCISME study, errors, be they large, small, administrative or clinical, were described as events in your practice that make you conclude: “That was a threat to patient well-being and should not happen. I don’t want it to happen again.”
The first-level classification included “process errors” and “knowledge and skills errors” (Fig 3-2). This 80/20 distribution was common to all countries and patient harm was reported in approximately 30% of cases. The detailed findings are shown in Table 3-2. It is the experience of the authors that a similar distribution applies to general dental practice.
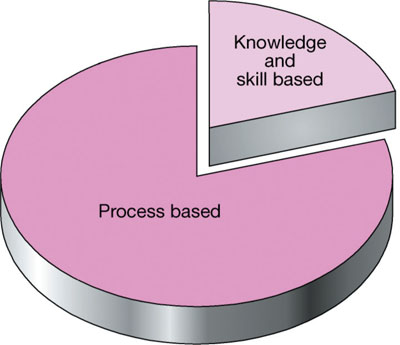
Fig 3-2 The 80/20 distribution of error types found in the PCISME study.
| Process-Based Errors |
| Errors in office administration: filing system incomplete charts patient flow (through the healthcare system) message handling appointments errors in maintenance of a safe physical environment. |
| Investigation errors: laboratory diagnostic imaging errors in the processes of other investigations. |
| Treatment errors: medication errors in other treatments. |
| Communication errors: dentist v. patients dentist v. other healthcare providers (non-medical) dentist v. physicians errors in communication amongst the whole healthcare team. |
| Payment errors: processing insurance claims electronic payments charging for care not received. |
| Errors in healthcare workforce management: absent staff not covered dysfunctional referral procedures errors in appointing after-hours workforce. |
| Knowledge- and Skills-Based Errors |
| Errors in the execution of a clinical task: non-clinical staff made the wrong clinical decision failed to follow standard practice lacked experience or expertise in a clinical task |
| Errors in diagnosis: error in diagnosis by a nurse delay in diagnosis wrong or delayed diagnosis due to misinterpretation of &n/> |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


