Bruxism is an oromandibular condition characterized by 2 distinct circadian manifestations, sleep bruxism and awake bruxism. Bruxism may be protective for obstructive sleep apnea. Bruxism can have significant implications for restorative dentistry, in terms of failure of natural teeth and dental restorations. Bruxism may also have specific implications in various dental specialties such as prosthodontics, endodontics, orofacial pain, and implantology, amongst others. Thus, bruxism may necessitate recognition and management through an interdisciplinary approach.
Key points
-
•
The concept of bruxim has significantly changed over the last several decades.
-
•
Bruxism is currently not considered as a disorder but rather as a muscle behavior, affected by various underlying conditions.
-
•
Bruxism can be protective with respect to obstructive apneic episodes.
-
•
Bruxism is a significant concern due to its impact on occlusal wear, failure of restorations, and temporomandibular disorders.
-
•
Bruxism can be managed by interdisciplinary approach.
Abbreviations
| AASM | American Academy of Sleep Medicine |
| AB | awake bruxism |
| CAs | clear aligners |
| EMA | ecological momentary assessment |
| EMG | electromyography |
| MMA | masticatory muscle activities |
| PSG | polysomnographic |
| SB | sleep bruxism |
| STAB | standardized tool for the assessment of bruxism |
| TMDs | temporomandibular disorders |
Introduction
Definition
Bruxism is a much debated oromandibular condition characterized by 2 distinct circadian manifestations, viz., sleep bruxism (SB) and awake bruxism (AB), and various activities of the jaw muscles (ie, grinding or clenching of the teeth and/or thrusting or bracing of the mandible). ,, The prevalence of AB is approximately 30% globally , and that of SB is about 6% to 8%. In the past, bruxism was diagnosed as possible , probable , or definite according to the methodology of assessment, but it is now clear that current knowledge on evaluation strategies and criteria is insufficient. ,,,
Where We Are Right Now: Evolution of the Concept
The construct of bruxism has significantly evolved over the past decades, to the point that bruxism is now conceptualized as an umbrella term to indicate a multifaceted phenomenon that requires standardized assessment methods. Originally, the Glossary of Prosthodontic Terms by the American Academy of Prosthodontics categorized bruxism as a parafunctional grinding of teeth. The American Academy of Sleep Medicine (AASM) incorporated bruxism into sleep medicine, classifying it first as a parasomnia and later as a sleep-related movement disorder (2005 International Classification of Sleep Disorders [ICSD]-2nd edition). This shift recognized that bruxism is more than a mere parafunctional habit, and related it to a patterned movement during sleep and linked to arousals. In medicine, bruxism was classified as sleep-related repetitive jaw muscle contractions, confirming its tonic and phasic variations. In this scenario, the need to find a common language has progressively emerged. Bruxism has been defined as an umbrella term denoting a multifaceted spectrum of masticatory muscle activities (MMAs), during wakefulness and sleep. ,,
Over time, concepts about the etiology of bruxism have drastically shifted away from early occlusion-centric consideration, which primarily linked it to occlusal discrepancies, occlusion-related habit, and stress. ,, The etiology of bruxism is currently recognized as multifactorial, ,,, involving a complex interplay of peripheral, psychological, genetic, environmental (ie, medication), and systemic factors.
In an attempt to provide homogeneity to bruxism evaluation, assessment approach has also been reconceptualized with the creation of the Standardized Tool for the Assessment of Bruxism (STAB). The STAB framework advocates for multiple domains, including self-reported (ie, questionnaires and history taking), extraoral and intraoral examination, instrumental assessment methods (ie., electromyographic or ecological momentary assessment [EMA] approach for AB and polysomnographic [PSG] recordings for SB). In addition, the STAB framework proposes to consider not only the presence or absence of MMAs but also the potential risk factors, comorbid conditions and potential clinical consequences. According to this new perspective, bruxism should not be considered a disorder but rather a muscle behavior that can be the sign of or be associated with various underlying conditions. Further, it can be harmless, harmful, or even protective with respect to several health outcomes. , For example, bruxism could serve as a protective mechanism during sleep apneic events or could consist of a physiologic response to stress or anxiety during wakefulness.
Fig. 1 illustrates the milestones in the evolution of the concept of bruxism.
Historical and recent milestones in the evolution of the concept of bruxism.
Implications for dental specialties
Both AB and SB have broad implications across multiple dental specialties, necessitating recognition and management through an interdisciplinary approach. , For dentistry, bruxism is a significant concern due to its impact on occlusal wear, failure of restorations, and temporomandibular disorders (TMDs). Appliances and bio-behavioral management may be appropriate. Episodes of SB can serve as red flag for diagnosing underlying comorbid conditions. For example, sleep specialists should evaluate the patients presenting with comorbid conditions, such as obstructive sleep apnea (OSA), and manage them accordingly.
Bruxism, Prosthodontics, and Restorative Dentistry
The negative clinical impacts of bruxism on the dental and supporting structures and restorations are well documented in the literature. Anecdotally and literature-wise, these may include but may not be limited to fractures, attrition and failure of restorations, amongst others. , The implications of these effects of bruxism in restorative dentistry can be frustrating for the reconstructing dentist, with the associated risk of increased stress, loss of time and finances. The restorative dentist should proactively screen the patient for evidence and existing effects of bruxism. The STAB framework can be instrumental in this regard. Any associated comorbidities such as snoring and OSA should be screened for as well. The clinician may want to carefully consider other special restorative materials and types of restorations. ,,, These may include shear-resistant porcelain and full porcelain restorations instead of porcelain-fused-to-metal restorations. It may be desirable to consider these factors and incorporate the possible complications into the informed patient consent. In the interest of protecting the clinicians’ and the patients’ investment in the executed treatment, it may be advisable to fabricate a full coverage occlusal guard once the restorative treatment is completed. Further research is necessary to elucidate the exact effects of bruxism and how to mitigate them.
Bruxism and Periodontics
Hardly any robust association was found in the literature regarding the effects of bruxism on periodontal tissues and conditions. As scanty as the literature appears to be, most of it is either anecdotal or proposed/hypothesized . There was no significant association found between periodontitis and bruxism. , On the contrary, bruxism has been shown to be associated with better periodontal health. The former concept of buttressing bone formation being associated with bruxism has been negated in the literature. There is no current evidence of any other significant association between bruxism and periodontal conditions.
Bruxism and Implants
The effects of bruxism on dental implants are inconclusive in the current literature. However, the plausible and proposed effects have been narrated. , SB is currently thought to cause implant fractures. , Association between bruxism and implants seems to be inconsistent across studies.
Bruxism and Endodontics
Excessive and repetitive MMA can lead to root and crown fractures. Bruxism may enhance fractures/failures of endodontically treated teeth. Abfractions may result from bruxism, with resultant dentin sensitivity potentially requiring additional treatment.
Bruxism and Temporomandibular Disorders
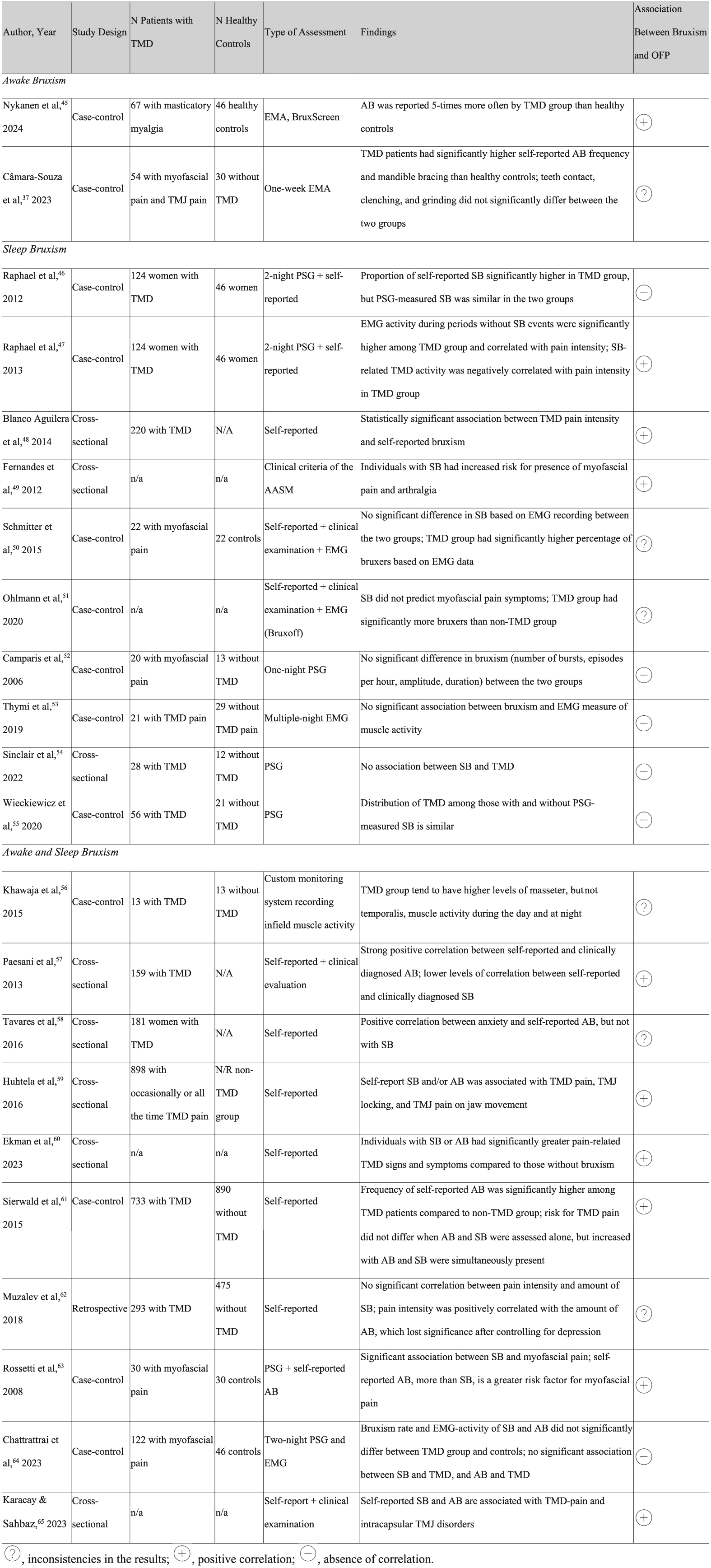
TMDs refer to a group of conditions that encompass muscle and intra-articular disorders. Bruxism is often suggested to be a potential cause of painful TMD-related pain. On one hand, studies conducted with objective measures, such as PSG and electromyography (EMG), have often revealed a lack of significant difference in the frequency or intensity of bruxism between TMD patients and healthy controls; on the other hand, a recent study conducted with EMA approach highlights that TMD patients have higher AB frequency than healthy individuals, and such manifestations are mainly characterized by jaw bracing. This is in line with early findings suggesting that self-reported bruxism is associated with TMDs, and an association between repetitive, low-level, long-lasting, nonfunctional muscle activity has been reported to be causing muscle fatigue and pain. This means that PSG/SB criteria, which are based on the count of masseter EMG events associated with sleep arousals, may provide only a partial picture of the complex range of jaw-muscle activities. ,,
Oral appliances may be beneficial in managing masticatory musculoskeletal pain in a bruxer. When a bruxer has pain in the temporomandibular joint (TMJ) or associated structures, it is prudent to explore the possible systemic factors that may contribute or perpetuate the pain and make the pain refractory.
In summary, the evidence is not yet conclusive, and further studies using objective measures and frequent real-time assessments are needed to determine the precise relationship between bruxism and TMDs. Taken altogether, this suggests that other factors, including but not limited to psychological stress, poor sleep, comorbidities, and other nonpainful musculoskeletal symptoms may play significant roles either in the development and maintenance of TMDs and bruxism. ,,
Table 1 provides a list of studies supporting or failing to support an association between bruxism and TMDs.
Table 1
Relationship between TMDs and bruxism in the literature ,,,,,,,,,,,,,,,,,,,,,
|
Abbreviations: n/a, not available; OFP, orofacial pain.
Bruxism and Orthodontics
Although older traditional orthodontic literature refers to a causal relationship between malocclusion and bruxism, the current literature seems to completely negate this philosophy. In these contexts, orthodontic treatments have also been suggested to reduce the frequency of self-reported bruxism. Yet, most of the evidence derives from cross-sectional or case-control studies, which are limited in their inability to draw definite causal temporal conclusions or may introduce recall and self-reported bias, which may impact finding reliability. Moreover, bruxism was mostly self-reported, which may lead to overestimated frequency. In contrast, many other studies and systematic reviews have failed to support any relationship between bruxism and malocclusion, ,, although there may be some evidence that those with bruxism had higher likelihood of presenting with crowding. Self-reported bruxism in patients undergoing an orthodontic treatment has been associated with 3-fold higher risk of presenting with TMDs. Occlusal appliances in general, transiently reduce bruxism activity, only to resume to preappliance frequency and intensity within approximately 3 months. ,
Concerning orthodontic treatment with clear aligners (CA), recent studies conducted with EMA approach and EMG highlight that dental professionals and orthodontists have suggested that the use of CA does not affect the sleep and awake bruxism activity, with minor exceptions related with interindividual differences. ,,
Bruxism and Pediatric Dentistry
Prevalence of bruxism in pediatric population has been reported variably depending on factors such as the definition used, diagnostic criteria, and the population. , The prevalence of SB accounts for 6% to 50% according to studies based on self-report or parental report. ,, In children, bruxism can be either primary (without an underlying medical condition) or secondary (associated with a medical condition). Common comorbidities of bruxism in the pediatric population include, but are not limited to, sleep disorders (OSA and restless leg syndrome), neurodevelopmental disorders, and syndromes. ,, In particular, some sleep disorders and parasomnias seem to be associated with parental-reported SB in children. The pediatric dentists are in a particularly unique position in the assessment of bruxism. Nasal obstruction, mouth breathing during daytime or nighttime, limited tongue mobility, and tonsillar hypertrophy were significantly associated with a diagnosis of probable SB in over 91% of the children.
Nevertheless, no consensus exists on the most appropriate and effective management strategies for bruxism in the pediatric population. , If an underlying condition is suspected, an interdisciplinary approach of pediatricians, sleep specialists, pediatric dentists, and orthodontists can help manage and address the underlying cause. In presence of a sleep related-disordered breathing diagnosis, effective management options to reduce the frequency of SB may include tonsillectomy and adenotonsillectomy. , Rapid palatal expander, when clinically indicated, has been suggested to significantly reduce snoring and self-reported SB episodes. , Available management options of bruxism in the pediatric population are illustrated in Fig. 2 .
Available assessment tools and possible management options of bruxism in pediatric patients.
Clinics care points
-
•
The concept of bruxism has significantly changed over the last several decades.
-
•
Bruxism is not considered as a disorder.
-
•
Bruxism is considered currently as a muscle behavior, affected by various underlying conditions.
-
•
Bruxism can be protective with respect to obstructive apneic episodes.
-
•
Bruxism is a significant concern due to its impact on occlusal wear, failure of restorations, and temporomandibular disorders.
-
•
Bruxism can be managed by interdisciplinary approach.
Statement of institutional review board approval or waiver
Institutional review and approval were not necessary for this manuscript.
Funding statement
None.
Disclosure
D.C. Thomas, D. Manfredini, A. Colonna, and L. Sangalli declare no conflict of interest.
References
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


