Highlights
- •
Angiolymphoid hyperplasia with eosinophilia (ALHE) is a benign vascular lesion.
- •
Therapeutic management can be challenging considering the frequency of recurrence.
- •
Despite surgical excision remaining be the most effective treatment option, ALHE has a recurrence rate of 44,2%.
- •
It is essential to carry out examination of the complete margins of the surgical specimen.
1
Introduction
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an uncommon benign vascular lesion, characterised by proliferation of small to medium-sized vascular structures lined by plump epithelioid (histicytoid) endothelial cells surrounded by a mixed inflammatory infiltrate [ , ]. Although its aetiology and pathogenesis are still uncertain, some authors [ , ] have suggested that ALHE represents a heterogeneous group of benign vascular lesions and reactive or reparative vascular proliferation.
The lesions of ALHE vary in clinical appearance from intradermal papules to subcutaneous nodules, may be solitary or multiple, red to brown in colour, quite small in size and usually occur in young adults [ ].
The lesions primarily occur in the skin and subcutaneous tissues of the head and neck [ ], particularly in the pre-auricular area and scalp, although some authors have also reported muscle, bone and salivary gland involvement [ ].
Surgical excision is considered the most effective treatment for this rare condition. However, it is suboptimal, as it is also associated with the highest rate of treatment failure versus other modalities such as administration of intralesional corticosteroids [ ], cryotherapy [ ], laser cauterisation [ ], and treatment with oral retinoids [ ] or pentoxifylline [ ].
Intraoral lesions of ALHE are uncommon [ ], and tongue involvement is extremely rare. A review of the English literature through a PubMed database search indicated that only 12 cases have previously been reported [ , ]. Here, we report an aggressive case of ALHE of the tongue, along with a review of the relevant literature.
2
Case report
A 60-year-old woman was referred to the Department of Maxillofacial Surgery of the University of Turin for evaluation of a painless lesion on the left lateral border of the tongue ( Fig. 1 ). The lesion had already been biopsied elsewhere, and the results of histological examination indicated granulation tissue, hyperplasia, acanthosis and parakeratosis of the epithelium without dysplasia. Detailed evaluations revealed an accidental bite 1 year previously following which the patient noticed the swelling, which became enlarged very slowly until reaching the condition at presentation.

Physical examinations revealed a whitish, lobulated, non-tender mass on the middle one third left lateral border of the tongue, measuring 13 mm at the greatest dimension. The soft to firm mass was not attached to the adjacent structures and was therefore mobile. Digital pressure did not elicit pain. There were no associated medical findings or a relevant family history of any other concomitant diseases. No regional lymphadenopathy was palpable.
A new preoperative incisional biopsy was carried out and microscopic features were similar to those of the previous sample. Two weeks later, the patient underwent surgical resection of the mass under general anaesthesia. Intra-operative examination of frozen sections revealed a specimen of muscular tissue with mild interstitial fibrosis and chronic inflammation, without evidence of malignancy. The lesion was extended up to about 1 mm from the surgical margins. The patient was discharged from the hospital 2 days after the surgery without any complications.
Macroscopic examination of the specimen revealed a whitish 3.0 × 2.0 × 1.5 cm mass that was soft to firm, with a white lobular greyish surface. Microscopic examinations indicated proliferation of vascular structures lined with epithelioid-like endothelial cells, with vesicular nuclei that protruded into the lumina and large vacuolated acidophilic cytoplasm. A dense cellular inflammatory infiltrate surrounding the vessels, which consisted mostly of eosinophilic granulocytes, was observed ( Fig. 2 a, b, 2c). No mitosis or nuclear atypia was found, and surgical margins were unimpaired. Immunohistochemical investigations using antibodies against CD31, a marker of endothelial differentiation, showed intense positive staining of numerous vascular structures ( Fig. 2 d).
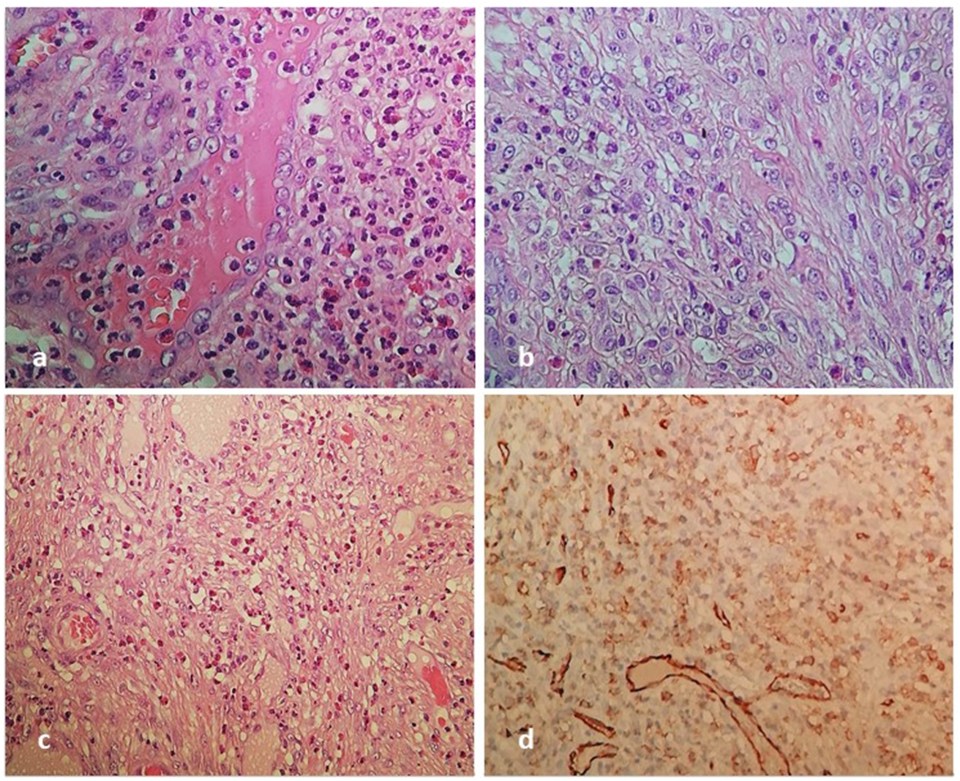
Based on the microscopic and immunohistochemical findings, the lesion was ultimately diagnosed as ALHE.
The lesion recurred in the same area 2 months after the operation with the same clinical appearance, measuring 10 mm in the greatest dimension. Therefore, a second attempt at surgical resection of the mass under general anaesthesia was made, with removal of about 3 mm of tissue from the lesion. At an 8-month follow-up, the lesion had recurred in the same area once again, measuring 8 mm in the greatest dimension. As the patient refused further surgical treatment, she was followed up on an outpatient basis. The lesion has since remained unchanged for 1 year.
3
Discussion
ALHE was first described by Wells and Whimster [ ] in 1969, while the term epithelioid haemangioma (EH) was proposed by Enzinger and Weiss [ ] in 1983 to describe the same lesion. Many other terms have been applied to these lesions, including inflammatory angiomatous nodule, pseudo- or atypical pyogenic granuloma and histiocytoid haemangioma [ ]. However, the term ALHE is the most commonly used nomenclature for these lesions in the English literature.
Intraoral lesions of ALHE are uncommon and the most frequent anatomical site is the lip, followed by the tongue and buccal mucosa [ ]. Tongue involvement is extremely rare, with only 12 cases reported to date ( Table 1 ), consisting of eight males and four females ranging in age from 23 to 82 years (mean, 52.5 years).
| Sex | Age | Lesion | Size a | Location | Preoperative diagnosis | Treatment | Recurrence | |
|---|---|---|---|---|---|---|---|---|
| [ ] | M | 31 | macule | 1,0 cm | left sublingual region | NS | excision | no for 1 year |
| [ ] | M | 82 | ulcer | 2,0 cm | right dorsal surface | squamous cell carcinoma | spontaneous remission after incisional biopsy | no for 6 months |
| [ ] | M | 48 | nodule | 3,0 cm | left ventral surface | NS | excision | after 5 weeks |
| [ ] | F | 43 | nodule | 1,0 cm | midline | NS | excision | no for 3 years |
| [ ] | M | 23 | ulcers | 1,0 cm and 0,4 cm | left lateral border | malignant tumor | excision | after 3 weeks |
| [ ] | M | 56 | ulcer | 1,5 cm | right lateral border | NS | excision after incisional biopsy | no for 6 months |
| [ ] | M | 59 | nodule | 4,3 cm | right posterior one-third and floor of mouth | Rhabdomyoma | excision | no for 2 months |
| [ ] | M | 52 | nodules | NS | NS | vascular tumor | excision | NS |
| F | 65 | nodule | NS | NS | pyogenic granuloma | excision | NS | |
| F | 32 | ulcer | NS | NS | squamous cell carcinoma | excision | after 3 months | |
| M | 48 | nodule | 1,5 cm | bottom | vascular tumor | excision | NS | |
| [ ] | F | 75 | ulcer | 0,5 cm | right lateral border | NS | excision | no for 1 year |
| Current study (2020) | F | 59 | nodule | 1,3 cm | left lateral border | malignant tumor | excision | after 2 months and 8 months |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


