CONSERVATIVE DENTISTRY
2.1 LASER AS DIAGNOSTIC TOOL
Fatima Zanin – Marina Consuelo Vitale
In the last years, incidence of dental caries, especially in paediatric dentistry, is decreased and we have assisted to a change of clinical carious manifestations due to the prevention politics. This reduction is due to several factors: sensibilization of mass-media, preventive dentistry with systemic and topic fluoride, periodic check-ups, applications of sealants.
The purpose of dental visit is to evaluate the clinical evidence and to recognize the potential problems.
Early diagnosis of carious lesions is one of the most important strategies of prevention in dentistry. Visual examination associated to the dental explorer is the most widespread method for a clinician to decide which therapy, restorative or preventive, should be chosen.
Nevertheless, the anatomical nature of pits and fissures gives a certain difficulty for a correct diagnosis of caries in the occlusal surface, especially when we have the so called “Hidden Caries”. The term of “Hidden Caries” is used to describe such lesions that are not clinically diagnosed using accepted visual-tactile criteria such as cavitation, softening, opacity, colour change, and they are detected only by x-ray examination as radiolucent lesions in dentin. The “Hidden Occlusal Caries”, developing deeply in pits and fissures of the dental occlusal surfaces, could be easily undetected, because sound enamel could cover demineralised tissue. This is one of the effect of fluoride-containing toothpaste and it is changing the pattern of the disease process: cavitation occurs later and the carious lesion in dentine may progress beneath a clinical intact enamel surface. So, we assist to a decrease of caries prevalence, but to an increase of occlusal caries proportion.
Many Authors (1-11) affirm that a primary carious lesion in pits and fissures is not recognized in 15 to 40%. In fact, the traditional methods for diagnosing pit and fissure caries (visual inspection and probing with a sharp explorer, x-rays, enamel colour, transillumination, endoral videocamera) may be of questionable accuracy in the correct diagnosis, especially in very early detection of carious process.
Different Authors (12-21) recommend the use of only visual examination in traditional method, because probing could be potentially damaging to the integrity of enamel surface, transfer and/or inoculate cariogenic micro-organism from one tooth to another.
In 1998, an alternative diagnostic device was commercialized: a diode laser, emitting red light, with a wavelength λ 655 nm (22-24). It evaluates fluorescence coming from dental surface, sound or demineralised tooth and it is able to quantify early mineral loss from dental caries (25-30). (Fig. 2.1.1)
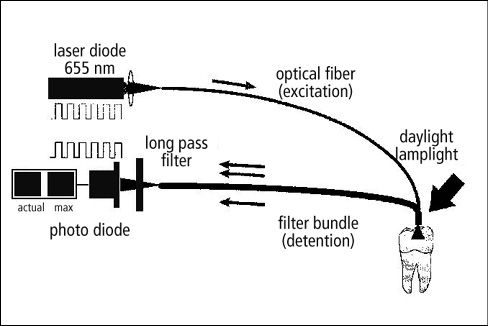
Figure 2.1.1 • Diagnodent System.
The first commercialized laser for caries detection is constituted by a flexible photoconductor with a special probe. The electric alimentation is provided by batteries, localized in the posterior part of the device. Diode and electronic instrumentation are inside (Fig. 2.1.2).

Figure 2.1.2 • The first Diagnodent, commercialized in 1998 and its characteristics.
Laser light is projected on dental surface by the flexible photoconductor and the probe. The fluorescence emitted by decayed tissues is capted by optical fibres located around the photoconductor tube. In the front, there is a display divided in two parts: on the left, the current value of measurement is indicated, on the right, the maximum value. Values are from 0 to 99.
Before using, it’s very important proceed to calibration and it is realized by a ceramic disc.
Diagnodent is provided by two different kinds of probes: one is trunk-conical for interproximal surfaces and the other one is flat for the occlusal surfaces.
Probe is located on the examined dental surface and the resulted values are directly proportionally to the gravity of the carious lesion.
The new Diagnodent is similar to a pen (Fig. 2.1.3). Batteries are located in the pen-stick and the display is on the handle. The principle is the same: on the display there are two values: one is the peak value, the other one is the real value at the moment of evaluation. At the value of 06, an acoustic signal is produced. For values between 6 to 99, frequency of acoustic signal is higher when values are progressive bigger. Two types of fibre-optic tips are available for this new device:
- a tapered tip designed for dental fissures and approximal regions
- a flat tip for smooth dental surface
When the tooth is illuminated by laser light (λ 655 nm), this light is absorbed by inorganic and organic dental substances. In caries lesions, where minerals are replaced by water, light scattering is higher than in sound tooth: during the progression of a carious process, it is shown an increase in the amount of the fluorescent light.
Every tooth is provided by its own natural fluorescence. For this reason, after calibration of the fibre-optic tip, it’s necessary measure the fluorescence of a sound spot on a smooth surface of the tooth in order to know the baseline value of that tooth. This value is subtracted from the fluorescence of the site to be measured.
False-positive could result when calculus, plaque, composite filling materials, stains, toothpastes, polishing pastes are present on dental surface or when there is an hypomineralized non carious teeth.
For this reason, it is very important point out the chronological different steps before measuring (Figg. 2.1.4, 2.1.5, 2.1.6, 2.1.7):
- calibration
- cleaning of dental surface
- determination of natural fluorescence of sound dental surface
- continuous rotary movement of the probe tip along its axis during the measuring procedure
- reading of measurements
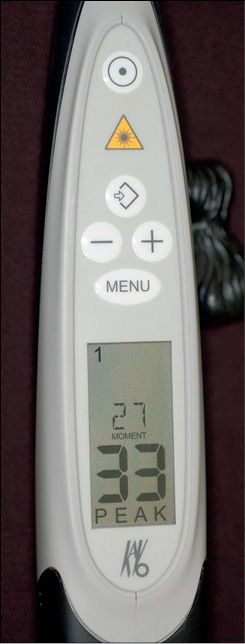
Figure 2.1.3 • The new diagnodent: Diagnodent Pen.

Figure 2.1.4 • Laser classification: laser class 1.

Figure 2.1.5 • Calibration.

Figure 2.1.6 • Calibration.
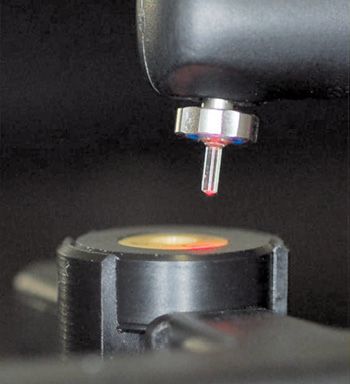
Figure 2.1.7 • Calibration.
For a correct reading, Lussi reported a guideline table 2.1.I for the clinical use of Diagnodent:
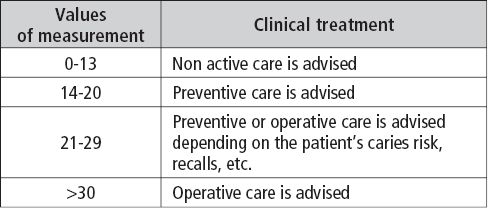
Table 2.1.I • Values of measurement of Diagnodent for a correct reading.
Because of its high sensitivity, the first laser fluorescence device was recommended as a tool in the decision-making process in r/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


