Chapter 13
REORGANIZED TECHNIQUES
As a general guide reorganized cases should be managed according to the stages listed below and shown diagrammatically in Figure 10-3. All of the stages are not necessarily required for every case, but the list does provide a basis on which to work, and often converts what appears to be a complex problem into a relatively simple one.
Stages
1) Stabilize the jaw and posterior tooth relationships.
2) Check.
3) Determine the anterior guidance.
4) Check.
5) Copy the anterior guidance.
6) Check.
7) Restore the posterior teeth.
Stabilize the Jaw and Posterior Tooth Relationships (Figs 13-1a–d)
By altering mandibulo/maxillary relationships, posterior deflective contacts and alterations in the vertical dimension influence the anterior relationships and hence the anterior guidance. It is not possible, therefore, to determine the definitive anterior guidance until the posterior relationships are stabilized. Conversely, it is not possible to establish the definitive posterior occlusal forms until the anterior guidance is established. It is necessary, therefore, to provide interim posterior stability preparatory to determining the anterior guidance.
This interim stability is usually provided on either amalgam restorations or provisional gold and resin restorations. In the latter case it is necessary initially to provide temporary restorations whilst the provisional restorations are fabricated in the laboratory (Chapter 8 and Appendix). Before making the interim restorations an occlusal stabilization appliance is often provided to eliminate the tooth determined proprioceptive reflex and enable diagnosis of deflective contacts. Occlusal adjustment, possibly leading to equilibration (Chapter 11) is then carried out, followed by interim restoration.
At this stage it is necessary to stabilize not only the jaw relationships, but also the teeth and periodontium, since instability in these structures will lead to instability in jaw relationships. Similarly, the problems of facial arthromyalgia must be managed (Chapter 26).
Check
The patient should feel comfortable and feel that there is simultaneous contact with even loading on posterior teeth when the jaws are closed together in both the supine and upright positions. There should not be a slide of the mandible when guided to CRCP closure and the patient asked to squeeze the teeth together. In CRCP, the posterior teeth should grip shimstock evenly, although if splinted via the provision of restorations, it is reasonable for some areas to be devoid of contact, provided that there is posterior and anterior contact on each section of the provisionals.
Determine the Anterior Guidance
(Figs 13-1d-g; 13-2a+b)
The contact relationships between the anterior teeth influence the pathways of mandibular movement. Criteria for acceptability of anterior guidance have been given in Chapter 10 (anterior occlusal schemes). When it is necessary to determine the anterior guidance on interim restorations they are usually made from either acrylic resin, or acrylic or composite resins on a gold substructure. The initial shape is produced with the aid of a celluloid slip made on a cast of a diagnostic wax-up and subsequently modified in the mouth to fulfil the clinical requirements of:
- Patient comfort.
- Aesthetic and phonetic acceptability.
- Unimpeded guidance.
- Minimal movement of guidance teeth.
- No increasing mobility of guidance teeth.
- No cementation failure of interim restorations.
Fig. 13-1 Reorganized technique.
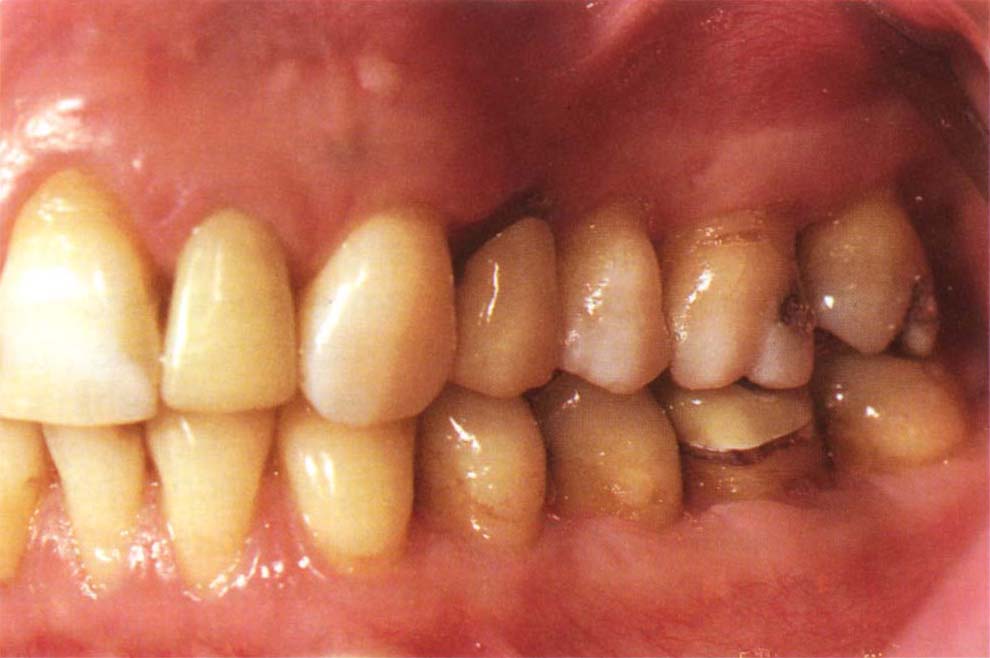
Fig. 13-1a Start.

Fig. 13-1b Casts in CRCP.
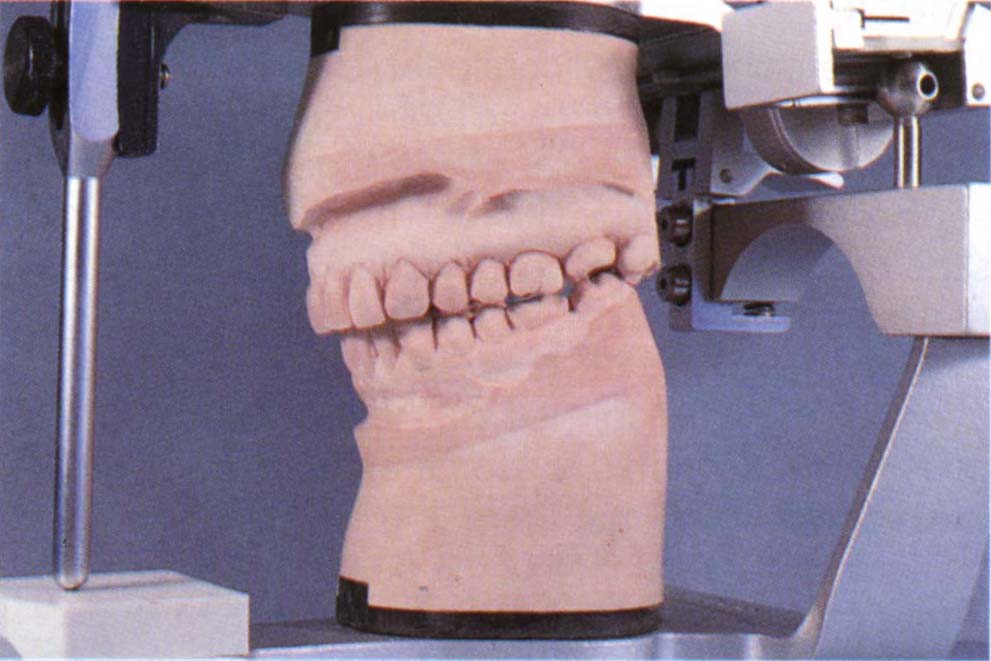
Fig. 13-1c Casts in IP. Initial therapy consisted of occlusal stabilization appliance, followed by PRI and muscle checks. When the PRI was indicating no dysfunction and there was no muscle sensitivity – occlusal equilibration to stabilize jaw relationships. PRI and muscle sensitivity re-checked.

Fig. 13-1d Tooth 28 was extracted. The posterior teeth were prepared and temporary, then provisional restorations made (teeth 24–27). PRI and muscles were checked.

Fig. 13-1e The anterior (12, 13, 22, 23) teeth were prepared. Temporary crowns in place (22, 23). Note the provisional restorations posteriorly. PRI and muscles were checked.
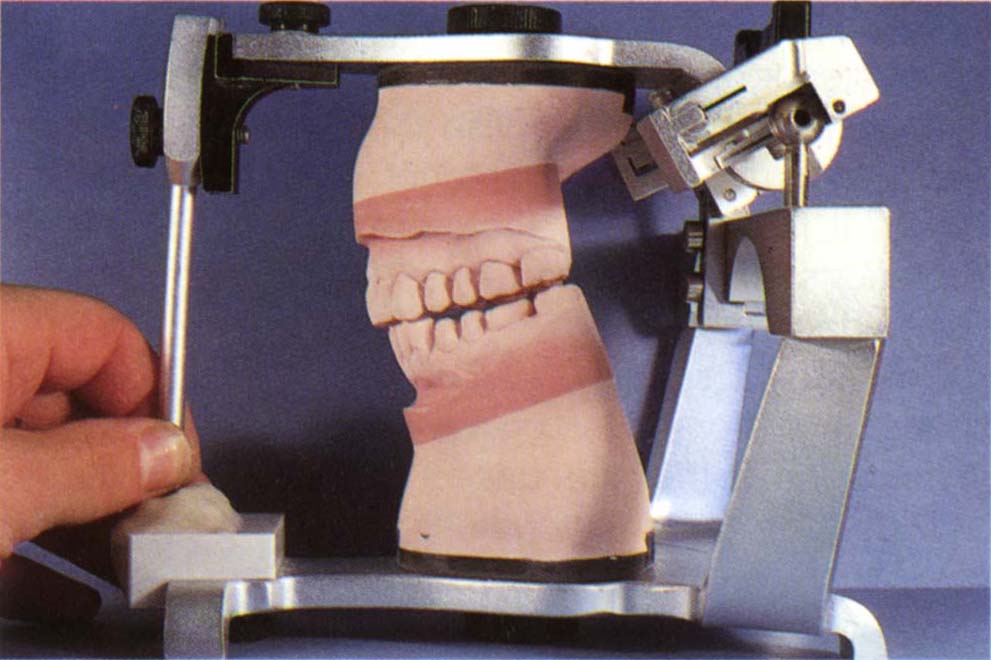
Fig. 13-1f Mounted cast of provisional restorations and anterior temporaries. Incisal guidance table made from this.
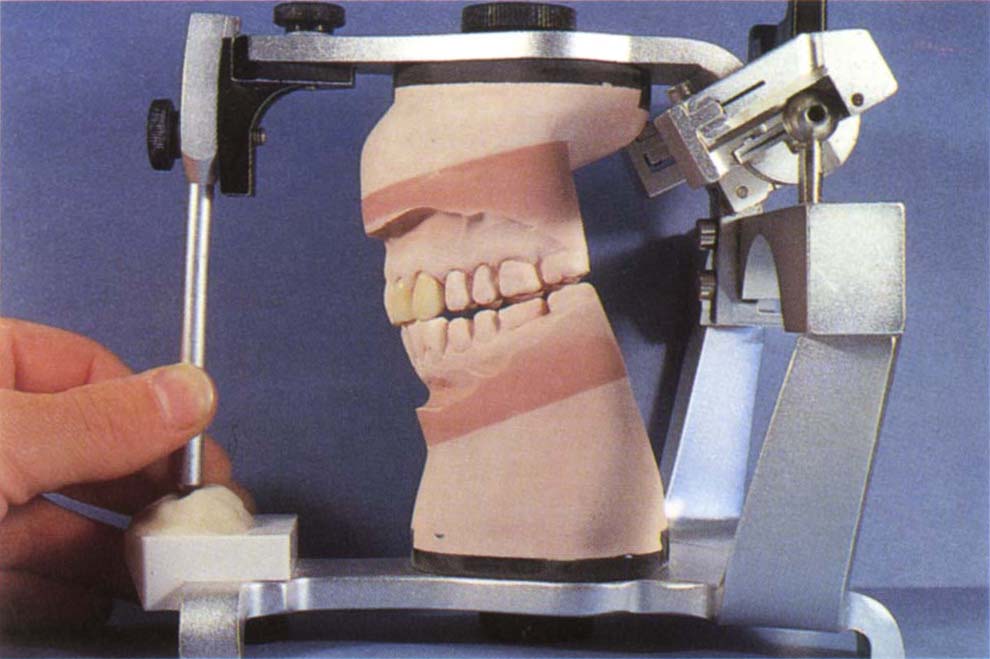
Fig. 13-1g Working casts. Interchangeable with the casts of the provisional restorations. Fabrication of the anterior porcelain restorations.

Fig. 13-1h The anterior crowns (13, 12, 22, 23), have been cemented and the posterior provisional restorations removed. The preparations were refined and new impressions made and jaw registrations made in CRCP at the correct vertical dimension, with 43–33 contacting 13–23, ensuring that there was no incline on the lingual of the anteriors deflecting the mandible nor labial movement, which would decrease the vertical dimension.
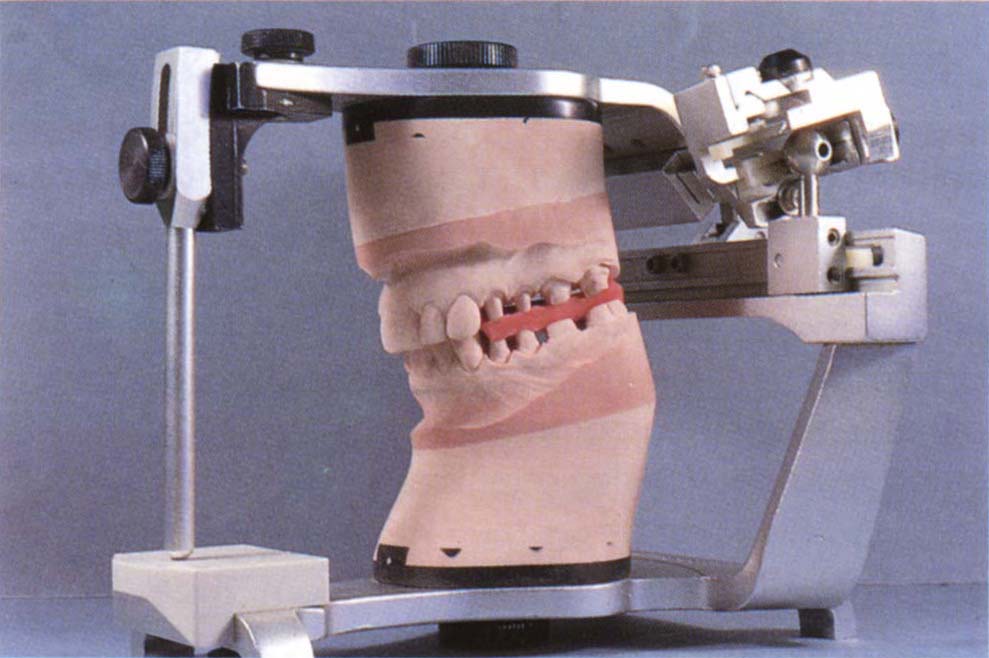
Fig. 13-1i The working casts were mounted using a facebow for the upper and jaw registration for the the lower. The mounting was checked with a Vericheck.
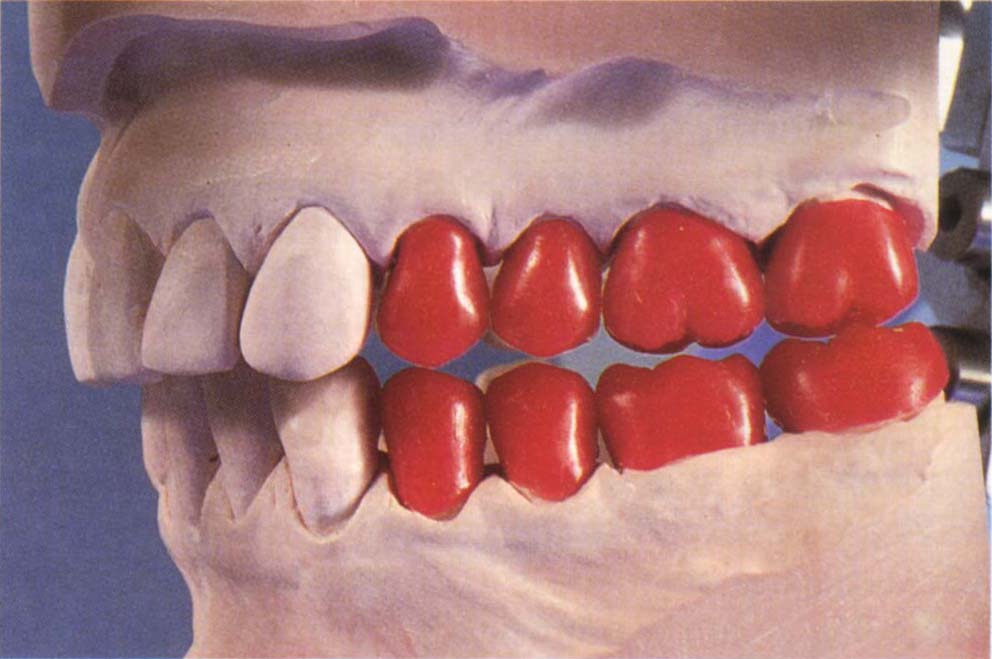
Fig. 13-1j Waxed up to full contour.
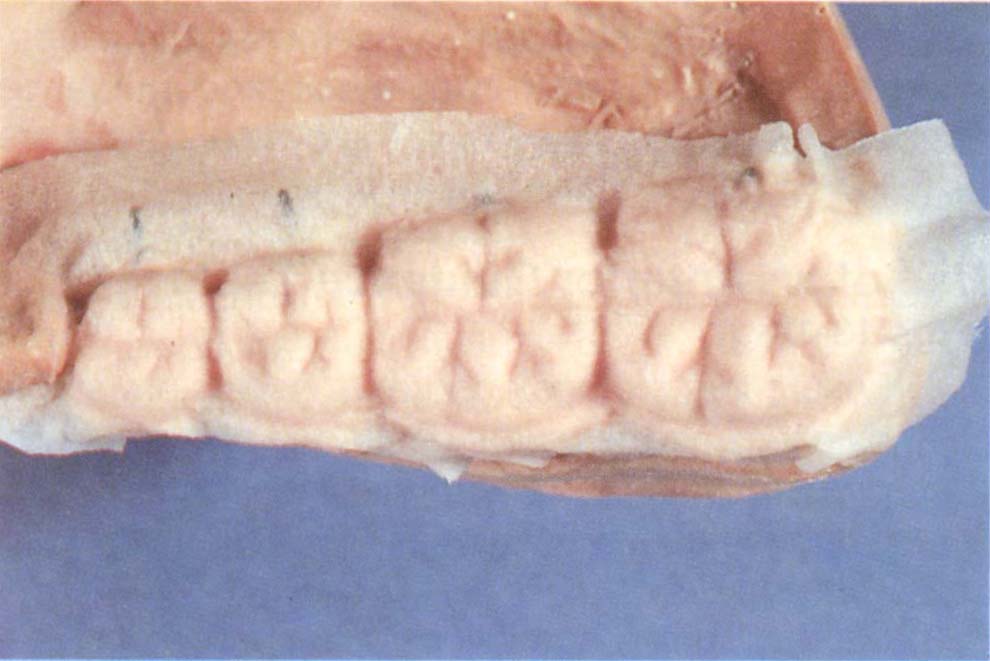
Fig. 13-1k Porcelain stamped out using an index made to the wax patterns (see Appendix).
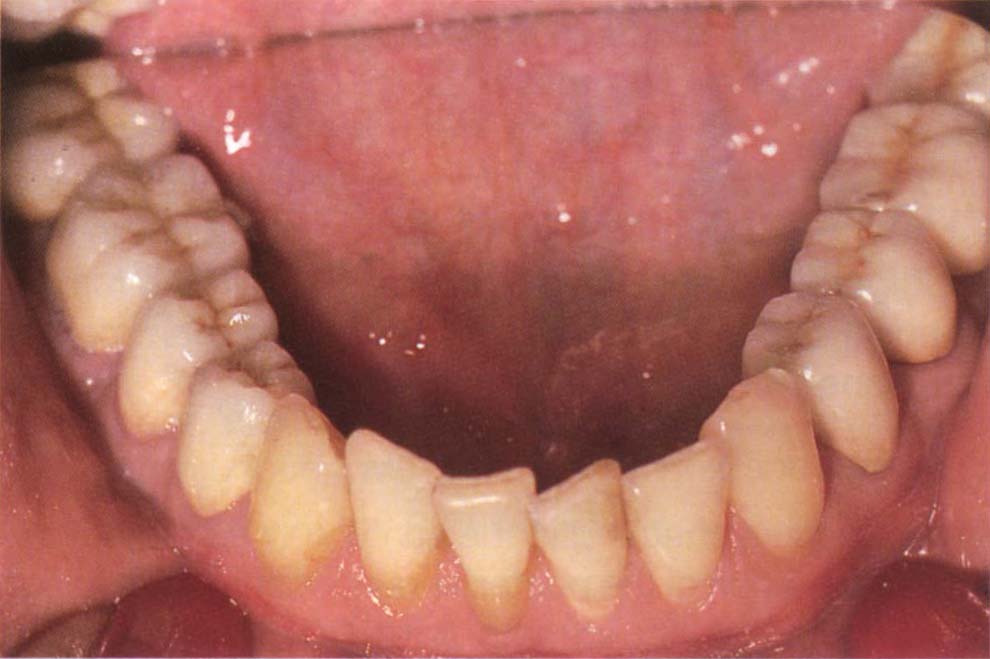
Fig. 13-1l Try-in of the lower completed porcelain and finish.
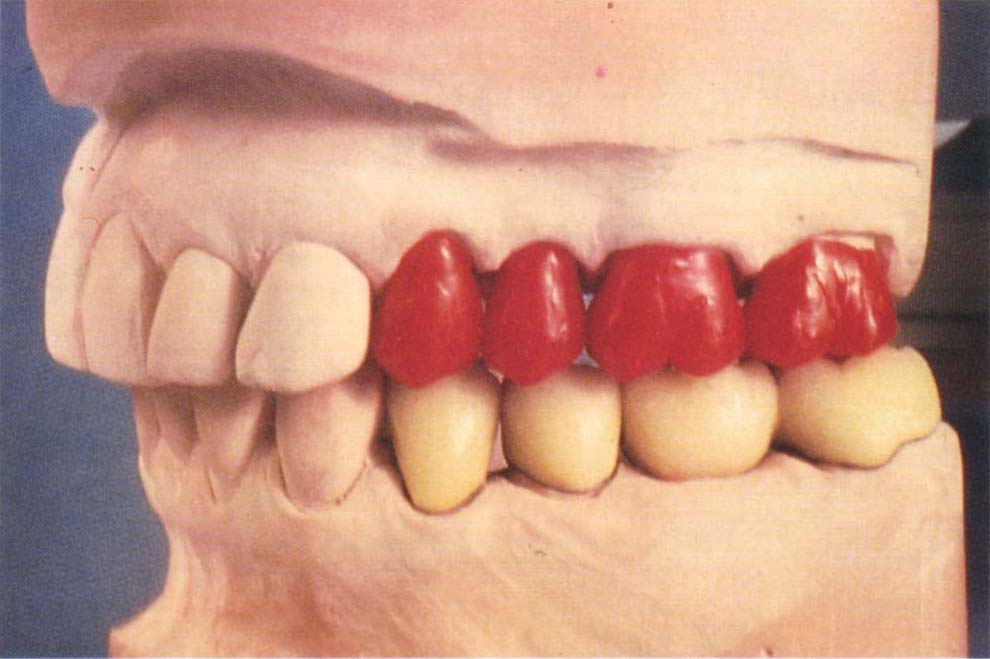
Fig. 13-1m The upper wax patterns are refined to the lower porcelain and then an index made and the upper porcelain stamped out. The intercuspal stops on the upper porcelain occlusal surfaces are slightly overbuilt and then refined against the lowers following firing. Try-in the mouth, adjust if necessary, glaze and stain.

Fig. 13-1n Finished upper porcelain (Patient’s finger in photograph).
Computer aided determination of anterior guidance angles may become more applicable in the future.
The restorations are tried in the mouth and checked for light centric relation contacts. Shimstock should just pull through between the anterior teeth, but be held between the posterior teeth. The patient is instructed to move the mandible in various excursions, and the requirements above are checked. Movement pathways are observed by the use of occlusal tapes (Figs 13-2a–b). The objective is to provide unimpeded contiuous fairly narrow pathways (approximately 1–2 mm wide), although the pathway does not necessarily have to be continuous along a single tooth. Sometimes the contact will change from, for example, the upper central incisors to the lateral incisors. Provided that this produces unimpeded guidance, it is acceptable. It is often helpful to place an index finger against the labial surface of the crowns so as to prevent any tooth movement or to feel which teeth are being displaced and, therefore, not marking correctly. Usually it is easier to begin with a slightly steeper guidance than anticipated, so that modification can be in the form of removal of plastic, which is much easier than making additions.
Check
The patient is checked in the same way as that following stabilization of the posterior relationship. In addition the criteria for acceptable anterior guidance listed above are rechecked and, if necessary, the guidance modified. There should be posterior disclusion in mandibular excursions. Muscles are palpated – sensitivity is an indication to delay definitive restoration. If available, a PRI is recorded. If this reveals dysfunction, definitive restoration is delayed. If definitive restoration is delayed, further adjustment to the existing restorations is made until the previous criteria are met. If they cannot be met, then future stages may become unpredictable in their outcome and more time must be allocated to cope with this eventuality.
Copy the Anterior Guidance
Having established the anterior guidance on provisional restorations, it is now possible to remove all except the posterior restorations and copy the form of the anterior provisional restorations. The definitive anterior restorations can then be cemented. The laboratory techniques used to copy the anterior guidance are described in the Appendix. The clinical stages are as follows:
Use of an Anterior Guidance Table
(Figs 13-1f+g)
1) Ensure that the posterior relationships are stable by checking the points described above. Do not proceed with the anterior segment until stability has been achieved.
2) Take shade.
3) Make full arch impressions of the provisional restorations and the opposing arch.
4) Make facebow transfer.
5) Make protrusive and lateral records, or pantographic records depending upon the choice of instrumentation.
6) Refine anterior tooth preparations and make the final impressions.
7) If the anterior teeth of only one arch are to be restored, make a jaw registration at the correct vertical dimension in CRCP, that is, with the posterior provisional restorations in contact. The working cast can then be mounted against the already mounted full arch opposing cast (Figs 13-1f–g).
8) If both upper and lower anterior teeth are to be restored then:
- Remove the upper anterior provisional restorations.
- Make a jaw registration in CRCP.
- Mount the upper working cast against the lower provisional cast.
- Remove the lower anterior provisional restorations and make a jaw registration to the upper anterior preparations in CRCP.
- Mount the lower working-cast to the />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


