Chapter 18
TELESCOPIC UNITS AND THE ADVANTAGES AND DISADVANTAGES OF FIXED/FIXED AND FIXED/MOVABLE BRIDGEWORK
Telescopic Units
Telescopic units, that is, individual copings cemented to the teeth with separate overcastings forming part of the overlying prosthesis, Figs 18-1a–c are used in both provisional and definitive restorations (see Appendix for details of fabrication).
Fig. 18-1 Telescopic units.
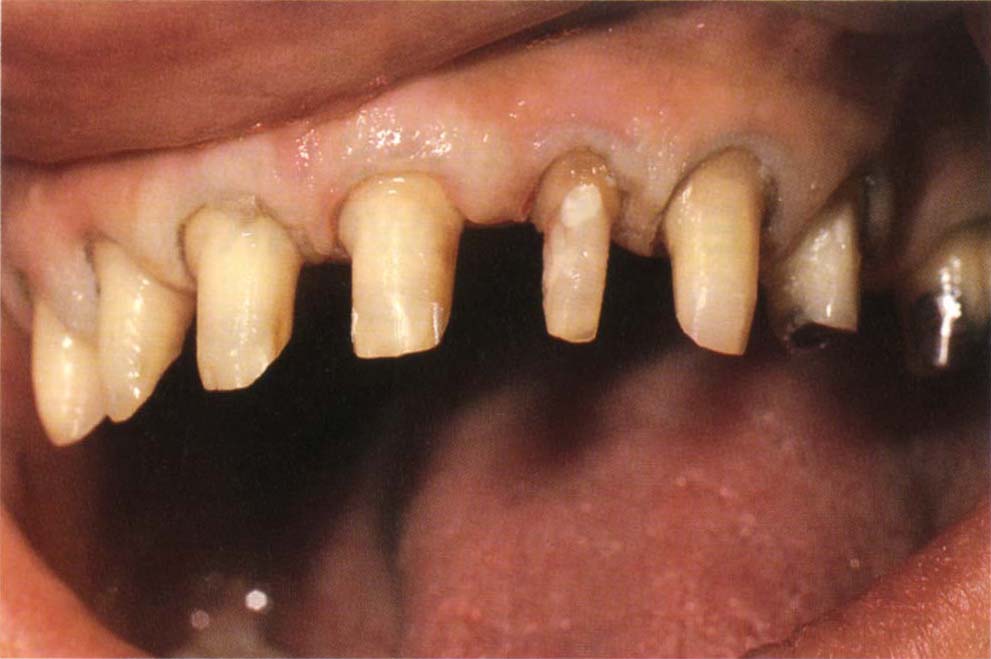
Fig. 18-1a The preparation must be adequate to provide space (retraction cord in place).

Fig. 18-1b Copings in place. The margins are polished, the remainder sandblasted. The margin has a narrow (approx. 0.25 mm) finish for the superstructure. Note that the contour of the coping allows sufficient space for the superstructure.

Fig. 18-1c Superstructure with posterior cantilevered units, teeth 14 and 15, cemented over the copings with Tempbond. The functional lip line covers the gold margins. Eight years following cementation.
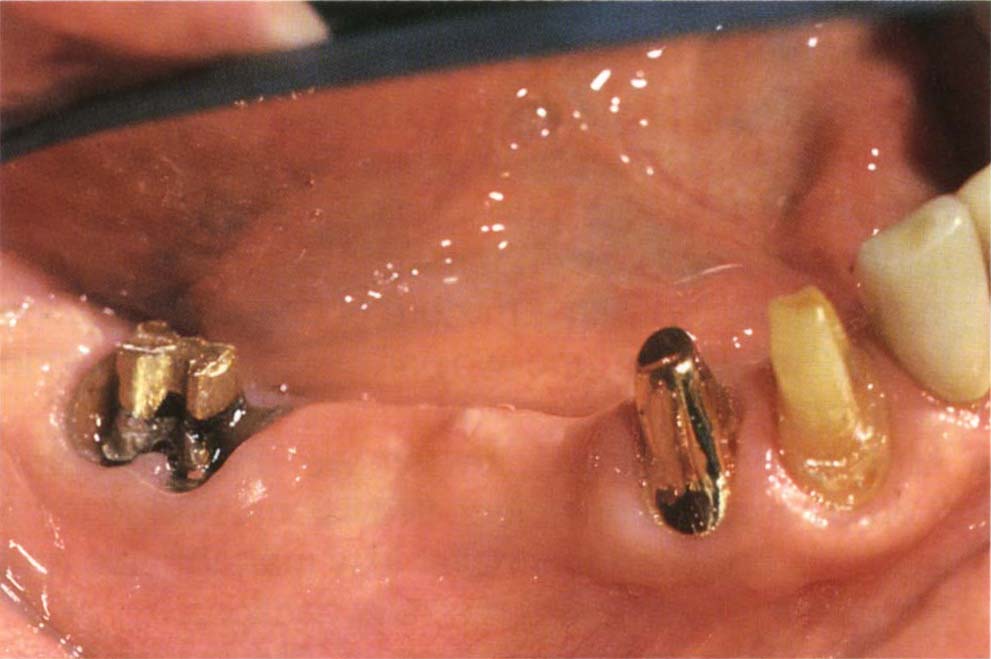
Fig. 18-1d Different mobility of abutments. The most mobile tooth moves out of the casting due to hydraulic pressure of the cement during cementation. There was cementation failure of the original bridge. It was not possible to remove the post in 47. 47 and 43 were non-mobile, but 44 exhibited grade 2 mobility. There was no pocketing, but 44 had lost attachment. A coping was placed on 44, so that when the bridge was cemented and 44 hydraulically displaced, the open margin would occur between the superstructure and coping and not the bridge and tooth.
Provisional Restorations
(see Chapter 8 for details)
- Telescopic units protect the underlying tooth stump in a caries susceptible patient. The coping is cemented with zinc phosphate, glass ionomer, or reinforced zinc oxide eugenol cement. The overcasting is cemented with a mixture of one part Vaseline from a 2 ml syringe, and two parts each of Tempbond base and catalyst.
- Align teeth. Copings can remove undercuts and thereby enable a one piece provisional bridge to be made as opposed to smaller less manageable and often less retentive and resistant sections.
- Provide isolation for endodontics. The coping is cemented with reinforced zinc oxide eugenol cement to provide an effective seal against leakage.
- Improve retention for provisional restorations. When the remaining tooth stump is very short, a coping which is longer and more parallel than the underlying stump can improve the resistance and retention form of the overlying provisional restoration, as it can be cemented with a stronger cement than that used for the provisional restoration, which must be readily removable. Using a temporary cement directly onto the short tooth stump can result in an unusable, provisional bridge as it constantly becomes uncemented.
Definitive Restorations
Telescopic units should be considered in the following cases:
- Different mobility of abutments.
- Long-span cantilevers.
- Minor tooth malalignment.
- Planning for future modification.
- Joining teeth and osseointegrated fixtures.
Different Mobility of Abutments
When rigid connectors are used between various components of long-span bridges, different mobilities of the abutment teeth may result in the most mobile teeth being hydrostatically depressed from the casting during cementation.1 This particularly occurs when two terminal abutments are non-mobile, but an intermediate abutment is mobile. The castings will seat on the terminal abutments, but the intermediate abutment will be depressed in its socket.1 Individual cementation of copings ensures that each coping has optimal marginal integrity. Cementation of the superstructure may lead to marginal discrepancies between this and the coping, but these are of no consequence (Fig 18-1d).
Long-Span Cantilevers
When long-span cantilevers are used with non-mobile abutment teeth, stress may develop, leading to mechanical failure, that is, fracture of the bridge, porcelain, cement or underlying tooth. With such restorations it is preferable to fabricate individual parallel copings for the abutment teeth and cement the superstructure with a mixture of Tempbond and Vaseline, as before. Stress concentration will result in cementation failure between the superstructure and coping, with dissipation of the stress and prevention of mechanical failure of the prosthesis (Chapter 19).
Minor Tooth Malalignment
Minor malalignment of abutment teeth can sometimes be overcome by fabricating copings to correct the malalignment. It must not be assumed that all malalignments can be corrected in the laboratory using copings. Excessive tilting will result in unacceptable overhangs on the coping and inadequate resistance and retention form (Fig 18-1e).
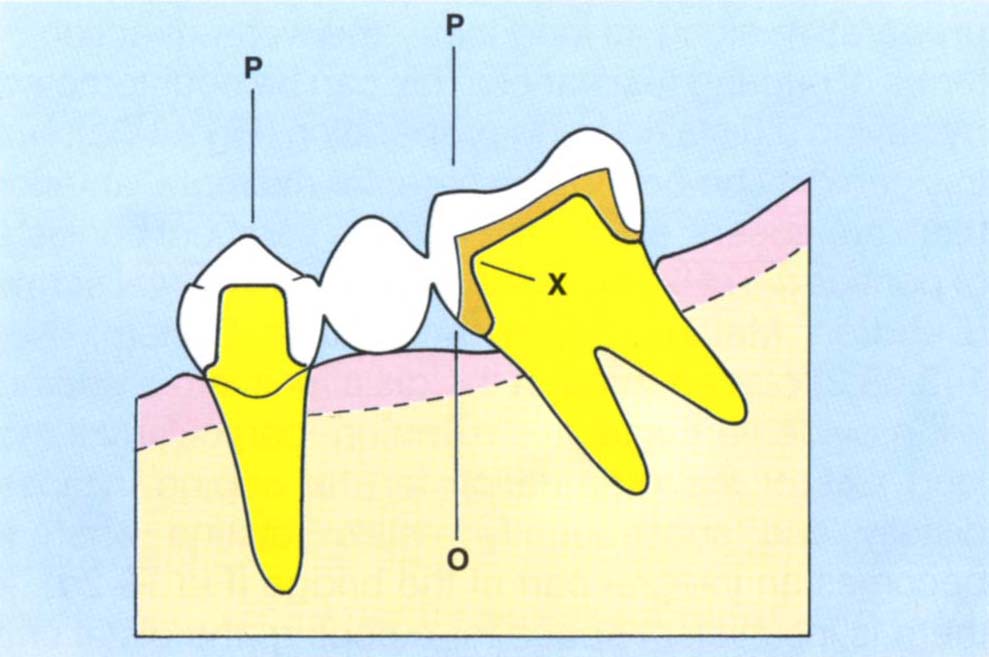
Fig. 18-1e Excessive tilting results in an overhang on the coping and overcrown 0. P = path of insertion parallel to the preparation on 35. The mesial and distal walls of the copings must be nearly parallel to this. Note that the mesial cervical dimension of the coping is dictated by the thickness at x.
Planning for Future Modification
The facility to remove the prosthesis in the event of failure is desirable, but not always necessary (Chapter 25). It is not desirable, however, to remove a temporarily cemented ceramo-metal bridge periodically from the underlying copings. This is difficult and may result in the fracture of porcelain or the underlying tooth stump.
The risk of cementation failure when using temporary cement can be reduced by incorporating screw devices (Cendres et Metaux Screw and Tube System No. 143.08.2) into the superstructure and underlying copings (Fig 18-1f).

Fig. 18-1f Sub-copings with horizontal Cendres et Metaux screw and tube (no. 143:08:2). The superstructure is cemented with Vaseline and Tempbond and screwed in place. The tooth supported section is not connected to the fixture.
Clinical experience gained from new patients presenting with failed bridgework, in the absence of precisely milled copings and temporary cement, is that screw retained bridges tend to fail through the loss of the screw, due to loosening under functional load.
Joining Teeth and Osseointegrated Fixtures
If teeth are joined to fixtures, copings over the teeth, cemented with zinc phosphate or glass ionomer cement, will facilitate cementation of the superstructure with a temporary cement. Hence the fixture supported section can be removed if necessary (see Chapter 33).
Fixed/Fixed or Fixed/Movable Bridgework
A decision must be made about whether the bridgework will be fixed or contain movable joints. The relative advantages and disadvantages of each system will be summarized. Each case must be individually evaluated.
Advantages of Fixed/Fixed Bridgework
- Forms rigid prosthesis.
- Ease of handling.
- Provides cross arch splinting.
- Resistance to rotation offered by distant units.
- More aesthetic as there is no attachment, which may show occlusally.
- Less tooth preparation required.
- The load is more widely distributed.
- Absence of joints which may wear.
Disadvantages of Fixed/Fixed Bridgework
- Possible bending of the bridge about intermediate abutments.
- Preparations must not be undercut relative to one another.
- Alters resistance form requirements.
- One piece casting or soldered.
- Different mobilities of abutments may result in open margins.
- All units have to be cemented simultaneously.
- No provision for future modification.
Advantages of Movable Joints within Bridgework
- Allows for flexure of the mandible.
- Load on the weakest retainers and abutments may be reduced.
- Permits reduction in occlusal coverage of minor retainer.
- Compensates for some abutment malalignment.
- Allows units to be cemented as individual sections.
- Allows individual movement of sections during function.
- Reduces cementation problems with abutments of different mobilities.
- May permit future modification.
Disadvantages of Movable Joints
- More space is required within the restoration.
- Metal may show occlusally at the site of the movable joint.
- Cannot always compensate for malalignment.
- Wear of joint will result in units becoming ‘cantilevered’, and so become functionally unacceptable or uncemented due to fracture of the cement.
- Sometimes there is insufficient crown height for a resistant attachment.
- Sometimes the tooth is too small for the extent of preparation needed, leading to bulbous crowns and closure of the embrasures.
When fixed/fixed bridgework is provided, the pontic is cast at one end onto a retainer and the other end is soldered using post ceramic soldering whenever porcelain units are incorporated (see Chapter 9). When movable joints are incorporated they are usually fabricated in the laboratory. See the Appendix for details. Obviously, preformed attachments can be used, but custom cutting facilitates a better contour to the restorations.
Each of the above will be considered in more detail.
Advantages of Fixed Bridgework
Rigid Prosthesis
Rigidity is required in cantilever bridges and where the degree of tooth mobility is functionally unacceptable. In these cases the prosthesis acts as a splint.
Ease of Handling
A rigid prosthesis is easier to handle th/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


