Chapter 23
ELECTIVE ENDODONTICS
When re-restoring teeth, it is often necessary to decide whether an apparently vital tooth should be endodontically treated, or whether to correct an existing root filling surgically. Obviously, pulpless teeth, with or without periapical signs and symptoms of pathosis, must be treated.
Instances in which Elective Endodontic Therapy of an Apparently Vital Tooth may be Justified
Many of the radiographic signs are subtle and radiographs must be observed carefully for:
- Pulpal exposure.
- Very deep caries or very deep existing restorations (Fig 23-1a), particularly if associated with any of the factors below.
- Overprepared tooth stump (Fig 23-1b).
- Sclerosing pulp canals, if the sclerosis were to continue non-surgical endodontic treatment might be impossible (Fig 23-1c).
- Hypercementosis (although this can be idiopathic) plus: (i) very deep caries; (ii) very deep restoration; (iii) overprepared tooth stump (Fig 23-1a).
- Blushing during tooth preparation (Fig 23-1d) which fails to disappear within one week when dressed immediately with a steroid paste, for example, Ledermix (Lederle), for 10 minutes and then with zinc oxide eugenol cement. This recommendation is based upon the clinical records of 35 such teeth observed, on average, for nine years, with a range of four to 16 years. Only one of the teeth has developed endodontic problems. This recommendation requires verification by controlled animal study.
- Apical root resorption or indistinct root outline and: (i) deep caries, (ii) deep restoration, or (iii) overpreparation (Fig 23-1e).
- Radiographic loss of cortical plate continuity, including any of the indications listed above (Fig 23-1f).
- Periapical sclerosis including any of the indications listed above (Figs 23-1c, e).
- Internal/external root resorption (Fig 23-1g and Fig 4-27e).
- Tooth stump with insufficient retention or resistance form (Fig 23-1b). A post and core may be required for a mutilated tooth stump.
- Parallelism problems that cannot be overcome without the fabrication of a post and core.
- Furcation problems requiring root resection or division.
- Continued pain following tooth preparation.
Fig. 23-1 Indications for elective endodontics.
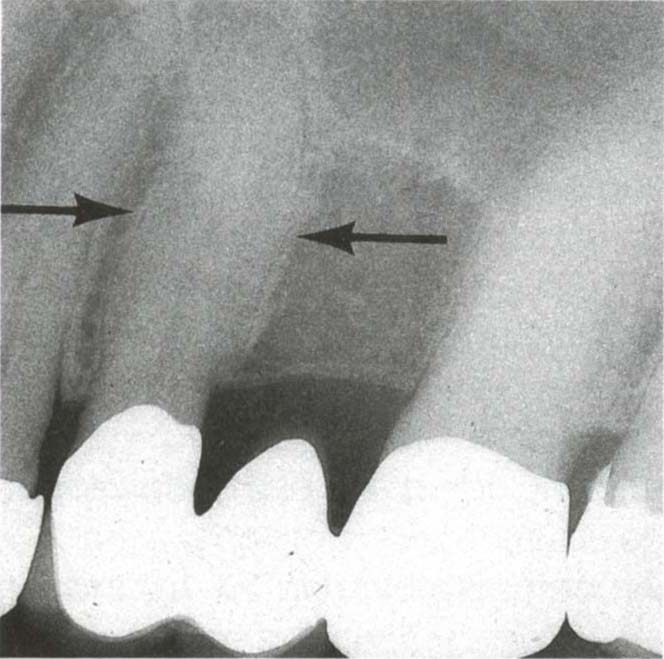
Fig. 23-1a Hypercementosis. The bridge did not need to be replaced and so the tooth was kept under observation. Two years later there was an acute pulpitis. If the bridge had needed to be replaced when the patient was first seen, then 25 should have been root treated at that stage.

Fig. 23-1b Over-prepared tooth stump. Removal of crowns reveals very short preparations which jeopardize the pulp and do not offer reliable resistance or retention form. Root filling and provision of posts and cores is indicated. Note that the posterior crowns have also been removed and, therefore, the anterior teeth are closer together than at the correct vertical dimension.
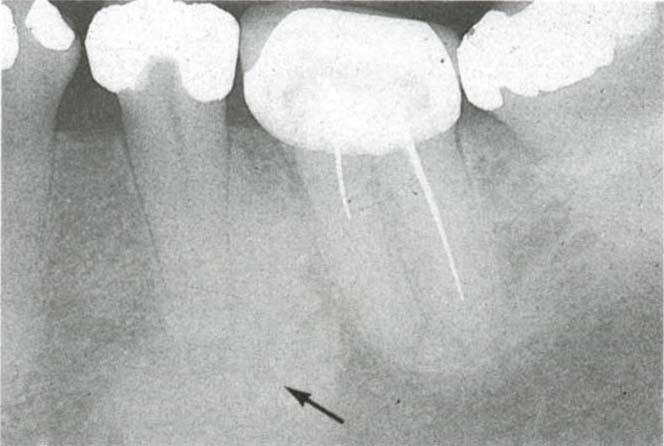
Fig. 23-1c Tooth 35 – deep restoration, distal caries, bony sclerosis (arrow). Tooth 36 – incomplete silver point root fillings with sclerosed canals. Re-restoration of mouth required. 35 should be root treated and 36 investigated.If 36 cannot be improved by either conventional root canal therapy or a surgical approach, then it should either be extracted or an attachment placed into the distal of 35 so that should 36 fail, it would be easy to remake the posterior section conformatively.

Fig. 23-1d Blushing during preparation. The pink hue of blood in the dentine can be seen on 13 and 14.
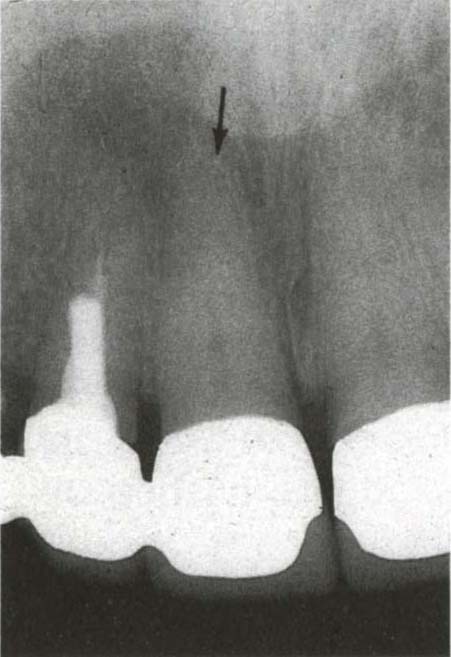
Fig. 23-1e There is blunting and shortening of the root apex of tooth 11, which is radiographically shorter than teeth 12 and 21. There is apical bony sclerosis. It is not possible to determine whether the periapical radiolucency is from tooth 12 or 11. Tooth 12 – the root filling is incomplete and poorly condensed and there is periapical radiolucency associated with 11 and 12. The post in 12 is close to the outer wall of the root. Removal would risk splitting or perforating the root unless the post can be removed easily by rotating between the fingers, then tooth 12 should be treated surgically and 11 with conventional endodontics prior to re-restoring the fractured bridge. 11 was non-vital with necrotic pulp remnants.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


