
An impacted canine should be given an opportunity to erupt into the oral cavity and serve its role as cornerstone of dental arch. Hence, the possibility of orthodontic repositioning of impacted canine should be explored before undertaking surgical removal of such tooth.
If the decision of the clinician is to undertake an orthodontic traction of canine after surgical exposure the following points have to be considered before attempting it.
Factors to be considered before attempting surgical orthodontic management of impacted canine are:
1. Favorably impacted canine.
2.Good patient cooperation for the long orthodontic and surgical approach.
3. No associated medical problems.
4. Good interdisciplinary support.
Determining the Favorability of an Impacted Canine for Orthodontic Treatment
Step1Assess whether the impaction is unilateral or bilateral.
Step2Clinically palpate for the buccal or the palatal bulge. If there is no bulge it might be in a mid alveolar position.
Step3Proper radiographs to confirm the buccolingual position and mesiodistal angulation should be made. Radiographic localization is described in Chapter 2. Intraoral periapical radiograph (IOPA) and occlusal radiograph are invaluable aids in deciding the exact position of the impacted canine.
Step4Locate the root apex of the impacted canine using radiograph (IOPA) and determine the root apex if the canine would have been normally erupted. Assess the difference in root apex location, the more it is deviated from the ideal apex mesially or distally the more difficult it will be to position. If the apex of the impacted tooth is close to the ideal apical position of the canine, it will be easier to position orthodontically. An assessment regarding the horizontal position also should be considered. Also if the incisal tip is displaced mesially more than the long axis of the lateral incisor it is again difficult to position.
Canines favorable for orthodontic eruption
•Labially positioned canines.
•Rootapex close to the normal apex.
•Incisal tip not displaced too much.
•Good patient cooperation.
Recently three-dimensional CT scans (Ericson S et al, 1988)’ have been used to precisely locate the impacted canine. They described the use of high-resolution computed tomography (CT) in the diagnosis of both the location and extent of root resorption of permanent incisors due to ectopic eruption of the maxillary canine. The CT image proved to be superior and more information was obtained than when conventional radiographic methods, including polytomography were used. Although CT is an expensive method, it is not timeconsuming or complicated. (Refer Chapter 2 for more details regarding use of CT scan).
Utilizing all the above diagnostic criteria the clinician should develop a mental picture about the possible placement of canine three dimensionally within the bone (almost similar to a 3D CT reconstruction image).
Bilateral, palatally placed and unfavorably angulated canines are usually difficult to position orthodontically but not impossible. Cost effort benefit analysis should be done before orthodontically attempting to position these teeth.
Good Patient Cooperation
Good patient cooperation (Becker A, 1998)2 is the key to success in surgical orthodontic positioning of impacted canine. The treatment time can vary depending on the placement and angulation of the impacted tooth. At times there can be bond failure during traction which may need further surgical opening and reattachment. The extra time required should be explained to the patient.
Associated Medical Problems
This aspect should be assessed as with any surgical case and necessary precautions should be taken to avoid complications. A risk benefit analysis should be made before attempting the surgical orthodontic positioning. If it is difficult to position the canine considering the medical condition, an alternative approach like surgical removal and replacement with prosthesis or leaving in its place may be considered.
Bilateral, palatally placed and unfavorably angulated canines are usually difficult to position orthodontically
Good Interdisciplinary Support
The need for surgical opening with minimal trauma and at the same time with maximum visibility and accessibility for bonding will need the service of an oral surgeon. Efficient orthodontic bonding, traction with directional control and precise aesthetic positioning may need the help of an orthodontist. Radiographic localization needs the support of a radiologist. Final gingival aesthetics may be enhanced by a cosmetic periodontist. Hence, all the concerned specialist should work in unison for the successful orthodontic management of an impacted canine.
Orthodontic Treatment Planning
a. Evaluate the space requirement for canine: This can be done by utilizing the mesiodistal width of the contralateral canine. Radiographs usually made of paralleling technique may be used in some cases especially for non rotated normally inclined canines.
b. Measures to gain additional space: Retained deciduous canines if present, might have maintained some space. Calculate any space that is present or possible means to gain it. Remember to create some extra space because there is every possibility to lose some space during the repositioning process.
Also determine whether additional extractions of premolars are required for correction of proclination along with impacted teeth, which should be based on facial aesthetics and occlusion status.
Orthodontic treatment planning
•Space requirement
•Space gaining measures
•Anchorage reinforcement
•Planning for correction of associated orthodontic problems.
c. Anchorage planning/reinforcement: Good anchorage source is very essential for successful positioning of canines (Becker A, 1998).2 The more unfavorable the tooth is, more the anchorage is needed. Unwanted movements of adjacent teeth should be expected and necessary steps to reinforce anchorage are essential. In case of bilateral impacted canines the anchorage requirement is more. A transpalatal arch or Nance palatal button may be considered to reinforce the molar anchorage. A molar distalization appliance could be considered to distalize the molar to create additional space in a non extraction case (Fig. 20.1).
d. Planning for correction of associated orthodontic problems: If the patient has associated problems like proclination or crowding along with impacted tooth, the question of which one to be carried out first will put the clinician in a dilemma. Waiting to complete one and then go for the other problems will unnecessarily increase the total treatment time. Here the clinician’s wisdom should be applied to carryout the entire process in a clinically justifiable short period.

Fig. 20.1: Creating space for canine positioning using intraoral molar distalization appliance
Orthodontic Treatment Strategy
The aims of orthodontic treatment for an impacted tooth are:
1.Provide a secure attachment on the crown to apply adequate force for its eruption.
2.Allow the tooth to erupt through the keratinized mucosa.2
3.Precisely position the tooth in the arch without compromising periodontal aesthetics.
The opening of space in the arch may initiate the movement of an unimpeded impacted tooth.2 By the time the space is adequate and the arrangement for surgery have been made, a new periapical radiograph may show a more positive change and often the clinician feels the tooth may erupt spontaneously.2 If it erupts by its own it is well and good, but if the eruption process is slow it is better to intervene surgically and initiate orthodontic traction.
The placement of orthodontic appliance carries some amount of risk to the tooth in terms of caries and periodontal problems. Every clinician should aim and attempt to finish the treatment in the shortest time frame to avoid this risk factor. When orthodontic treatment has created enough space to accommodate the impacted tooth, surgical procedures to remove any associated pathology as well as to initiate traction are to be undertaken simultaneously. If the pathology associated is a cyst or a space occupying lesion it may have to be treated initially and sufficient time should be given for healing and new bone formation. Here orthodontic strap up could be delayed to reduce the risk of periodontal damage.
Attachments
The placement of orthodontic attachment on the correct buccal side of the tooth crown is another important aspect in the interdisciplinary management of the impacted canine. Bonding an attachment to the crown could be performed either during the surgical opening (Becker et al, 1975)3 or can be performed several days or weeks later, i.e. an open method. Both have its advantages and disadvantages as detailed below. In a closed eruption or a full flap closure method, the attachment should be bonded on the same appointment.
Advantage of Bonding on the Same Appointment
a.A closed method of eruption which is superior to the open method could be carried out.
b.Bond strength is found to be superior as the newly exposed tooth is covered only with the enamel cuticle which is only one micron thick and could be easily removed by the application of the orthophosphoric acid used for etching.(Becker et al 1996)4
c.Healing could be achieved by primary intention.
One of the main disadvantages of bonding at the same appointment is the problem of moisture control during bonding.
Advantages of Bonding in a Second Visit
a.Dry field could be easily achieved, which is very critical for bond strength.
b.Appointment can be scheduled as per the doctor’s will and the long process of surgical opening and bonding at same visit could be avoided.
The disadvantages of bonding in a second visit are:
a.After few days of exposure of the tooth to oral environment there is plaque and food debris accumulation on the crown. This needs to be removed prior to bonding by polishing with rubber cup and pumice paste. If the opening is not wide enough adequate cleansing is difficult.
b.The edematous tissue may bleed which can result in poor bond strength.
c.The surgeon needs to create a wide opening to prevent the spontaneous closure and to facilitate polishing, which can affect the future periodontal health and aesthetics.
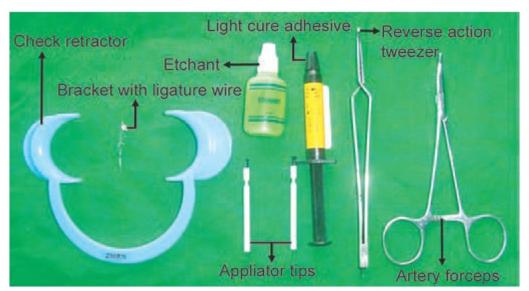
Fig. 20.2A: Armamentarium used for orthodontic bonding
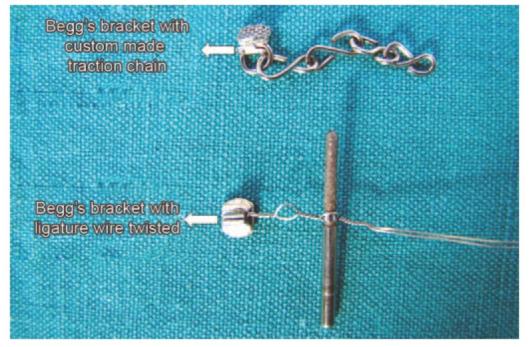
Fig. 20.2B: Begg’s bracket with custom made traction chain and ligature wire twisted
Armamentarium for Successful Bonding (Figs 20.2A and B)
1.The selected attachment with ligature tie.
2.Reverse action tweezer.
3.Orthodontic adhesive system comprising of phosphoric acid gel, bonding agent (if required as per the manufacture’s specification), and applicator tips.
4.Polishing cup and pumice paste.
5.Ligature director.
6.Artery forceps.
7.Elastic thread or chain depending on the mode of force application.
Procedure of Bonding (in the same visit approach)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


