

The instruments used for surgical removal of impacted teeth are essentially a combination of instruments used for transalveolar extraction and soft tissue surgery in the mouth. There are only a few special instruments that are required. Very often the selection of instruments is a matter of personal preference. The following description of instruments and equipment is intended for the guidance of the dental surgeon who is new in the field, since an experienced person will have his own concept of an instrument tray set-up. It is essential that the bare minimum instruments are used depending on the case with provision to meet exigencies. This is because a large collection of unfamiliar instruments and an elaborate tray set-up will cause embarrassment for both the patient as well the operator and interfere with efficient progress of the surgery. The instrument tray set-up can be considered under the following headings:
1. Local anesthesia
2. Instruments to incise mucoperiosteum
3. Instruments to reflect mucoperiosteum
4. Instruments to retract mucoperiosteal flap
5. Bone cutting/tooth division instruments
6. Instruments for irrigation and suction
7. Instruments for removal of tooth and debridement of surgical site
8. Instruments for closure of mucoperiosteal flap
9. Other equipment
1.Local anesthesia: Local anesthetic containing vasoconstrictor (e.g. lignocaine 2% with adrenalin) ensures adequate analgesia as well as reduces bleeding.
Moreover, it helps in defining tissue planes. Whether to use local anesthetic available in vials or in cartridges is a matter of individual preference. While operating under general anesthesia, use of local anesthesia can compliment the analgesia effect of the anesthetic. Hence, its use is recommended. However, it is essential to seek the permission of the anesthetist before injecting solution containing adrenalin since adrenalin in local anesthetic can precipitate cardiac arrhythmias when halothane or similar drug is used as the general anesthetic.
2. Instruments to incise mucoperiosteum: Usually No.15 scalpel blade on a No.3 Bard Parker handle is used for incising the mucoperiosteum. Some operator’s advice the use of the curved No.12 blade while making the posterior cut distal to the third molar and also for buccal cervical margin. If the pointed No. 11 scalpel blade is used care should be taken not to inadvertently injure the angle of the mouth or buccal mucosa.
3. Instruments to reflect mucoperiosteum: Mucoperiosteum is reflected using periosteal elevator. Howarth periosteal elevator which was originally designed for use as a nasal raspatory is an ideal instrument for reflecting the mucoperiosteum (Fig. 7.1). The sharp end of the instrument is inserted in the vertical component of the incision to verify that that the incision is down to the bone and the opposite broad curved end used for raising the mucoperiosteal flap. This instrument can also be used as a retractor of the mucoperiosteum on the buccal as well as the lingual aspect of the third molar.
Other periosteal elevators like Burser periosteal elevator (Fig.7.2) is useful in elevating the mucoperiosteum, the sharp end of the instrument is inserted into the incision margin of mucoperiosteum and the blunt end is used to elevate it. While a Freeier periosteal elevator (Fig.7.3) is useful in subperiosteal tunneling. A #9 Molt periosteal elevator (Fig.7.1) is most widely used for elevation of subperiosteal flaps and for completing dissection in all subperiosteal planes.
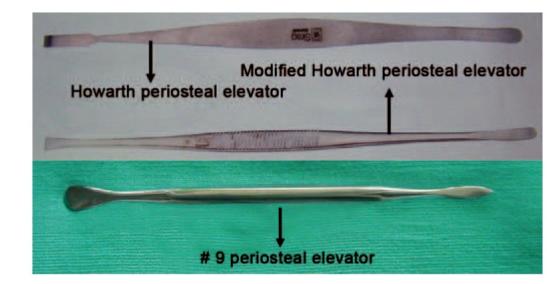
Fig. 7.1: Howarth periosteal elevators and #9 Molt periosteal elevator

Fig. 7.2: Burser periosteal elevator

Fig. 7.3: Freeier periosteal elevator
4. Instruments to retract mucoperiosteal flap: Numerous instruments are available for this purpose. The array of instruments available indicates that a perfect retractor has not been introduced so far.
Some of the useful retractors are the Austin’s retractor for retracting the flap (Fig. 7.4), Kilner retractor for holding the lip, Lack’s tongue depressor for retracting the tongue (Fig. 7.10) and Rowe’s lingual retractor. Malleable stainless steel/copper strips (Fig. 7.5) of varying width which can be bend to desired shapes are also useful instruments for retraction of the flap in third molar surgery. Retractors are now available with suction tip which help the operator to retract and at the same time aid in suctioning (Fig.7.9).

Fig. 7.4: Austin’s retractor

Fig.7.5: Stainless steel malleable retractor

Fig. 7.6: Minnesota retractor

Fig. 7.7: Cawood-Minnesota retractor
Other retractors now available are Minnesota retractor, Cawood-Minnesota (Figs 7.6 and 7.7) retractor for retracting the mucoperiosteal flap and Weider tongue retractor for retracting the tongue (Fig. 7.8). In addition to the above a number of other retractors (Fig. 7.10) are also available which aid in third molar surgery.

Fig. 7.8: Weider tongue retractor

Fig. 7.9: Austin’s retractor with attached suction tip
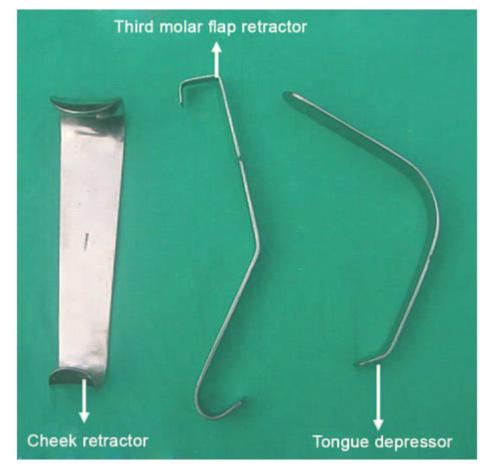
Fig. 7.10: Various types of retractors useful in mandibular third molar surgery
A flat bladed retractor should always be employed to hold the mucoperiosteal flap from site when bur is used to remove bone. Otherwise, the bur may injure the soft tissue flap.
5. Bone cutting/tooth division instruments: Chisel and bur are used for the removal of bone. It is a debatable issue as to which is the ideal one among these two. Chisel has the advantage of rapidity, no production of heat and no generation of bone dust. It is a quick clean method for removing young elastic bone. However, while operating under local anesthesia use of chisel and mallet is an unpleasant experience for the patient. Hence, it is best avoided and the instrument of choice then is bur. Nevertheless chisel is an excellent instrument for use while doing surgery under general anesthesia. In cases where the mandible is thin and atrophic or when the bone is brittle or sclerosed as in old patients it is prudent to use bur since injudicious use of chisel can result in splintering of bone or fracture of mandible. Similarly, when the access is limited for the use of chisel as in case of a deeply impacted tooth, bone removal is best accomplished by use of bur. Use of bur has the disadvantage of generation of heat and bone debris during drilling. Both these can be avoided by the use of continuous irrigation and suction. It is important to note that the handpiece should never be introduced or taken out from the patient’s mouth while the bur is still revolving due to the possibility of causing inadvertent injury to the soft tissues.
A rational approach will be selection of the chisel or bur technique depending upon the case or a combination of the two.
Use of chisel and mallet: The chisel should be preferably of 5 to 6 mm width with tungsten carbide tip with sharp edge (Fig. 7.11).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


