The nose is the most prominent feature of the face and has little protection from trauma. It is the most easily fractured of the facial bones and, not surprisingly, the most commonly fractured. Fractures occur twice as often in men as in women and are often the result of automotive accidents, interpersonal violence, or sporting injuries. One report indicates that more than one third of nasal fractures are associated with alcohol use.
Despite a relatively low incidence of facial fractures in children, an estimated 25% of nasal fractures occur in patients younger than 12 years of age. Fractures can occur in newborns due to malposition in utero and during birth, in infants and toddlers as a result of bumps and falls as they begin to crawl or walk, and in children and teenagers as they participate in competitive sports. Because the child’s nose is more cartilaginous than bony, fractures can be difficult to diagnose, and they frequently remain undiagnosed until a deformity develops with growth.
Repair of nasal fractures is a simple procedure, but it is associated with relatively high revision rates. Results of inappropriate treatment include cosmetic external deformity and internal nasal airway obstruction, with resultant snoring and sinusitis. Delayed or abnormal growth of the nose and midface and disturbance of the dentition can occur in children.
Classification
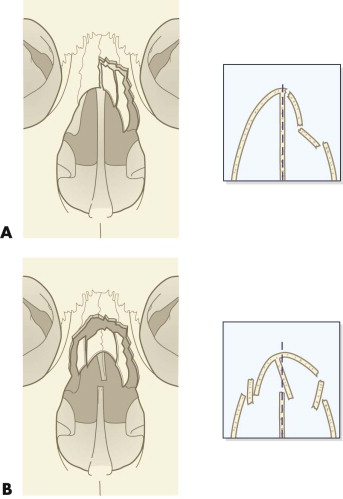
The type of nasal injury sustained depends on the age of the patient and the direction and intensity of the forces applied. Most nasal fractures in adults result from a lateral blunt force. Typically, the nasal bone and the frontal process of the maxilla are involved unilaterally ( Fig. 13-1A ). With greater force, bilateral displacement of the nasal bones is seen. Because the nasal bones increase in thickness from their inferior aspect upward toward the junction with the frontal process, most nasal fractures occur in the midsection below the thicker portion, with the base of the nasal pyramid remaining in situ. Frontal rather than lateral blows result in posterior displacement or impaction of the nasal bones. The fracture line is located along the midsection (see Fig. 13-1B ). More severe force disrupts the frontonasal suture, and as the impact force increases, nasal, orbital, and ethmoidal fractures occur in combination. In children, the relatively large amount of cartilage and open suture lines predisposes to an open book–type fracture, which results in a flattened appearance of the nose (see Fig. 13-1C ). The bony component of these fractures is classified as type I (simple unilateral), type II (simple bilateral), and type III (comminuted unilateral, bilateral, or frontal).
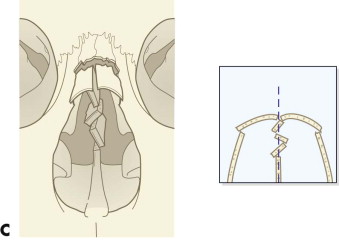
The septal component, the most important but often undiagnosed feature, requires accurate reduction and alignment if secondary deformities are to be avoided. The septum tends to follow the displacement of the nasal bone fractures, and the nasal bones tend to unite in the direction of the deviated septum. The extent of the septal injury determines the appropriate technique for septal correction. Lateral force results in displacement or a low fracture of the septal cartilage from the maxillary crest, producing a partial or complete obstruction on one side of the nasal cavity. The fracture dislocation usually occurs along the vomerine groove ( Fig. 13-2A ). Greater force, particularly when associated with frontal impact, may extensively fracture the septum in a more vertical direction through the thin central region of the quadrangular cartilage, which extends between the perpendicular plate of the ethmoid above and the upper edge of the vomer below (see Fig. 13-2B ). Most septal fractures result in some telescoping of the cartilages, loss of vertical central support, and widening of the base of the septum. The septal component of these fractures is classified as type IV (nasal bone and septal dislocation), which is subdivided into type IVa (associated with a septal hematoma) and type IVb (associated with an open nasal laceration).
Assessment
Understanding the mechanism and direction of the forces involved should provide an accurate three-dimensional mental image of the disrupted nasal anatomy. Examination includes a visual assessment of the nasal deviation, location of any lacerations, and assessment of the degree of swelling and bruising. Palpation may reveal specific areas of tenderness, crepitus, or a bony step. Simple nasal fractures should be differentiated from more complex facial fractures. Complex nasal fractures predominantly involve extension of the fracture into the nasoethmoidal complex. These fractures may be associated with much more serious complications, are more difficult to treat, and often are accompanied by other injuries, such as head injuries. For example, after the nasoethmoidal complex is fractured, there may be detachment of the medial canthal ligament or fractures extending into the frontal sinus or cribriform plate. These fractures require assessment with computed tomography (CT) and treatment by open reduction. The intercanthal distance may be increased in severe injuries, indicating a more complex nasoethmoidal injury.
An intranasal examination to determine the status of the septum should be carried out under adequate lighting and using a nasal speculum. A septal hematoma requires immediate evacuation. Decongesting the nose with a topical decongestant can be beneficial to the examination. A full endoscopic examination is advised for a complete assessment of the septum (particularly at the posteroinferior junction with the perpendicular plate of the ethmoid), turbinates, and inferior meati. This examination may have to be delayed until the operating room. Airway patency is in part determined by the patient’s own assessment of his or her breathing before and after injury.
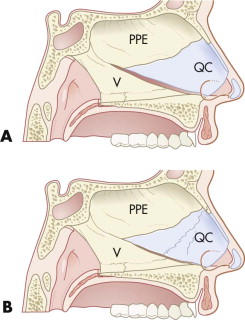
Radiographic examination, although routinely performed, is often of questionable value. Plain films are of little benefit other than for medicolegal reasons, because they are rarely helpful in determining the need for surgery or the type of surgical intervention required ( Fig. 13-3A ). A CT scan provides better information, particularly of the position of the septum and patency of the airway, but it is costly and does not replace a thorough history and physical examination, particularly if an endoscopic assessment is performed (see Fig. 13-3C ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


