Chapter 10
Indirect pulp therapy for young permanent molars
Patrice B. Wunsch
Introduction
Young permanent teeth differ from mature permanent teeth in that the roots of young permanent teeth are not fully formed. The duration for root completion in the permanent molars is 3 years after full eruption of the tooth (American Academy of Pediatric Dentistry, 2011). This may vary between patients; therefore, obtaining a diagnostic radiograph to include the roots of the teeth is recommended before initiating any type of pulp therapy to not only rule out the possibility of periapical pathology, but also determine the apical development of the tooth (Figure 10.1).
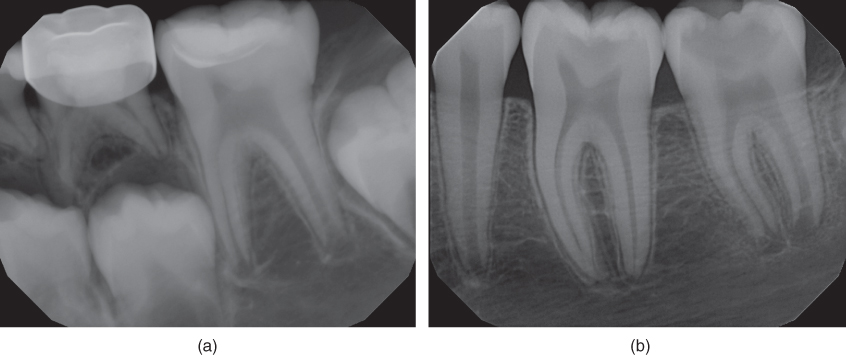
Figure 10.1 (a and b) Young immature permanent molars, note incomplete closure of the root apices (contributed by Dr. Claudia Colorado, VCU Department of Endodontics).
There are certain advantages of treating young permanent teeth with immature roots. The pulp biology varies in that permanent teeth with immature roots have a more viable pulp that will respond more favorably to insult and treatment therapies than permanent teeth with fully formed roots (Trope, 2008). This is discussed in greater detail under the treatment modalities section of this chapter.
Background
As the permanent molars erupt into the oral cavity, there is a likelihood that the pits and fissures of the occlusal surface are composed of uncoalesced enamel, meaning that the enamel surface is not intact and the potential for bacterial invasion of the dentinal subsurface is high. This in itself will predispose the tooth to develop a large carious lesion before the tooth has fully erupted into the oral cavity. In addition, the position of the partially erupted permanent molars places the tooth at risk for plaque accumulation. Sometimes, the molar is not in contact with the opposing teeth, thereby not allowing the self-cleansing action of the occlusal surfaces coming in contact. Also, young patients are not as efficient at brushing the posterior teeth compared to their ability to clean the teeth positioned more anteriorly (Antowson et al., 2012).
Indications for indirect pulp therapy on young permanent molars
In the event of deep caries in a young permanent tooth, the practitioner is faced with numerous factors that will affect the success of treatment.
- Patient behavior and level of cooperation.
- Preoperative symptoms.
- Apical development of the tooth.
In a patient who has minimal coping skills, indirect pulp therapy (IPT) is a viable option in that it allows one to atraumatically arrest the caries process until trust and cooperation are achieved or some other means of behavior management are successful in order to provide care. There is a two-step (stepwise) method of IPT that would lend itself well for the patient who has poor coping skills. The provider will initially use a spoon excavator to remove gross caries and food debris followed by the placement of a glass ionomer (GI) temporary restoration. This has been extremely helpful because not only does this treatment relieve the symptoms associated with the open lesion, but also affords the dentist time to schedule more definitive care at a later date. The medicament placed on the remaining caries changes the characteristic of the carious tooth structure that is left behind after initial excavation (Maltz et al., 2007; Orhan et al., 2008). The stepwise IPT technique is described later in this chapter under technique.
Diagnosis
A comprehensive review of the patient’s medical and dental history must be initially completed. The clinical examination includes an intraoral and extraoral examination of the hard and soft tissues associated with the area of the patient’s chief complaint. Radiographic examination to include a bitewing and periapical radiographs should be taken. The bitewing is used to evaluate the extent of the caries and its proximity to the pulp. The periapical radiograph is used to look for signs of periapical pathology. The tooth in question should have clinical tests such as percussion and palpation to assess for periapical pathology or mobility. Electric pulp testing and cold tests can be unreliable in young immature teeth with developing roots (Camp, 2008).
However, cold tests can be useful when the caries as noted on a radiograph approximates the pulp or when pathosis is noted on the periapical radiograph.
To differentiate between reversible and irreversible pulpitis, initial cold tests can be used to provide a baseline on which the tooth can be monitored for pulpal changes.
Indirect pulp therapy is indicated for teeth with signs of reversible pulpitis
Symptoms consistent with the diagnosis of reversible pulpitis include pain brought on by a stimulus (usually sweets or cold). The pain will subside after the stimulus is removed. Radiographically, the periapical film shows no signs of periapical pathology, and the bitewing film shows caries encroaching on the pulp but not into the pulp. Similarly to primary teeth, young immature permanent teeth do not respond reliably to electric pulp testing or cold tests. Therefore, the most reliable indicator for treatment is the history of symptoms and the clinical/radiographic examination.
Signs and symptoms consistent with a diagnosis of irreversible pulpitis are spontaneous pain, sensitivity to cold liquids or cold air, and radiographic signs of a widened periodontal ligament.
Signs and symptoms consistent with a diagnosis of necrotic pulp are spontaneous pain (patient wakes often at night in pain), swelling associated with the tooth, presence of a parulis, and often signs of a radiolucent lesion (periapical pathology).
Teeth that have a diagnosis consistent with irreversible pulpitis or a necrotic pulp are not candidates for IPT or other vital pulp therapies.
Young immature permanent teeth, due to their highly vascular pulp, have the potential to heal and withstand carious insult better than mature permanent teeth with fully formed roots (Ward, 2002).
As early as the 1960s, a comprehensive study was performed by the Eastman Dental Center. Investigators found “after histological evaluation of the teeth selected for IPT that had all caries been removed, pulpal exposure would have occurred. In addition, only 3% of 475 teeth treated with IPT resulted in frank clinical failure.” This study has demonstrated that clinicians should not aggressively remove all carious dentin in an effort to leave none behind and risk exposing the pulp (Ranly & Garcia-Godoy, 2000).
What is indirect pulp therapy (IPT)?
Indirect pulp therapy involves the incomplete removal of carious dentin. Cariously involved dentin is divided into two layers. The layer that is more coronal to the pulp is described as the infected layer or infected dentin. Contained within this layer are viable cariogenic bacteria. This layer is “dead tissue with both organic and inorganic components irreversibly deteriorated that is deemed infected and nonreminieralizable.” During the IPT procedure, this is layer is removed. The remaining layer that is in close proximity to the pulp is called the affected layer or affected dentin. Within the affected layer lay the “organic and inorganic components present with sound structure and character but are slightly and reversibly degenerated, uninfected, and physiologically remineralizable” (Orhan et al., 2010). It is this layer on which a biocompatible material is placed to aid in remineralization. In order for the procedure to be successful, the tooth must be sealed from bacterial invasion. It is recommended that the final restoration be one that would not allow for any leakage around the margins. With this in mind, sealing the final restoration has been shown to decrease or prevent marginal leakage, thereby improving treatment success (Mertz-Fairhurst, 1998).

Figure 10.2 Vitrebond and Dycal (contributed by Dr. Claudia Colorado, VCU Department of Endodontics).
Medicaments: glass ionomer (Vitrebond) and calcium hydroxide (Dycal) (Figure 10.2)
Dycal is available in hard-setting and light-cured forms. The high pH of the calcium hydroxide in Dycal has a bactericidal effect, and calcium hydroxide is able to induce mineralization (Foreman & Barnes, 1990).
GI is available as a liner or a restorative type. The most popular GI type is Vitrebond (3M ESPE). This lining material can be placed in close proximity to the pulp where its anticariogenic ability (due to fluoride release) is most effective.
GI restorative materials include Fugi II/IX (GC America), Ketac Molar (3M ESPE), and Photac Fil (3M ESPE). The GI restorative materials can be used as temporary restorations (stepwise technique) or as a base over the IPT as added protection for the pulp before the final restoration.
In general, GIs have been shown to inhibit the growth of cariogenic bacteria due to their ability to release fluoride.
How does fluoride affect certain oral bacteria in vivo?
Fluoride indirectly affects mutans streptococci (MS) by limiting their ability to produce acid and thereby preventing a decrease in pH (Hamilton, 1990).
Chronic exposure to fluoride may decrease the population of MS while increasing the number of more alkaline species (Hamilton, 1990).
GI releases a high concentration of fluoride after its initial application. Over time, the concentration of fluoride decreases, and therefore more importance is placed on the ability of the final restoration to create an adequate seal.
Both Dycal and Vitrebond are considered good lining materials for IPT in young immature permanent teeth. Marchi et al. have studied IPT in primary teeth. The authors believe that IPT is not a material-dependent treatment and that a good marginal seal of the final restoration and controlling the caries-inducing activities of the patient will ensure success (Marchi et al., 2006).
Indirect pulp therapy technique
After careful assessment of the radiographs (Figure 10.3) and preoperative symptoms, the tooth is anesthetized, and a rubber dam is used to isolate the tooth.
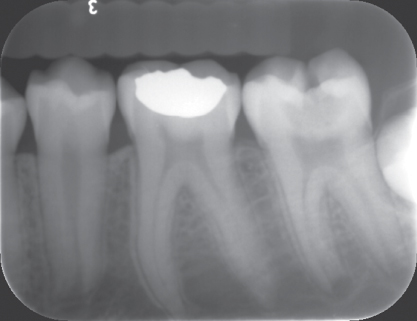
Figure 10.3 Preoperative radiograph of tooth #18 with deep caries and incomplete closure of root apex (contributed by Dr. Patrice Wunsch, VCU Department of Pediatric Dentistry).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


