Chapter 16
Space maintenance
Jane A. Soxman
Space maintenance may be necessary after premature tooth loss in the primary and mixed dentition to preserve arch length, width, and perimeter (American Academy of Pediatric Dentistry, 2014a). Space loss is considered to be one of the major contributors to malocclusion in the permanent dentition, along with ectopic eruption or impaction of premolars (Simon et al., 2012; Dean, 2012). For cases in which space loss has already occurred, such as with ectopic eruption of maxillary first permanent molars or space loss due to interproximal caries before extraction, appliances are used for space control. Preservation of the tooth with restoration or delaying extraction should be considered, understanding that the natural tooth is the best space maintainer. If orthodontic treatment is to begin within 6 months of primary molar loss or the permanent successor is near eruption, a space maintainer may not be necessary.
Sequence of eruption
Sequence of eruption, which may vary, should be considered when treatment planning for a space maintainer in the early and late mixed dentition. In the mandible, the first permanent molars erupt first, followed by the central incisors, lateral incisors, canines, first premolars, and second premolars. In the maxilla, the first permanent molars are followed by the central incisors, lateral incisors, first premolars, second premolars, and last, the canines. This sequence of eruption in the maxilla will be a consideration when managing ectopic eruption of the maxillary permanent canines (American Academy of Pediatric Dentistry, 2014b).
Dental age
Dental age and chronological age may differ. Typically, the permanent first molar erupts at the age of 5.5–7 years, and mandibular incisors erupt at the age of 6–7 years, but if eruption does not occur until the age of 8 or 9 years, the child is dentally delayed. This delay typically follows throughout the eruption of the permanent dentition. Conversely, if the permanent dentition erupts earlier than usual, the child is dentally ahead (American Academy of Pediatric Dentistry, 2014b).
Alveolar bone covering permanent successor
The amount of alveolar bone covering the permanent successor should also be considered. About 6 months is necessary for the permanent successor to move through 1 mm of bone, which can be determined with a bitewing or periapical radiograph (Simon et al., 2012).
Root development of permanent successor
Root length of the permanent successor should be evaluated. Premolars typically erupt when one-half to three-fourths of the root has formed (Terlaji & Donly, 2001). If the primary molar is extracted due to an abscess, the permanent successor may erupt more rapidly than expected with less root formation.
Time elapsed since loss of primary tooth
Space maintainers should be inserted within a few weeks after an extraction. Space loss usually occurs within 6 months after premature loss of a primary molar (Simon et al., 2012). Space loss typically occurs more rapidly in the maxilla than in the mandible. Inform parents/guardians that if too much time elapses before insertion, space closure may occur and the space maintainer will no longer fit. Another impression and laboratory fee for fabrication of a revised space maintainer will be necessary. If possible, obtain a photograph or radiograph of the site to document space loss before inserting the appliance.
Space maintenance appliances
Fixed appliances are preferable to removable, avoiding loss, breakage, choking, and noncompliance with wear. The band and loop or crown and loop are used for premature loss of a maxillary or mandibular first primary molar. For premature loss of a second primary molar, the Nance or transpalatal arch appliances are used in the maxillary arch and the lower lingual holding arch (passive lingual arch) are used in the mandible. Actual examples of appliances can be used for more detailed explanation along with a mixed dentition typodont (Kilgore International) (Figure 16.1).

Figure 16.1 Mixed dentition typodont (Kilgore International).
Problems with space maintainers
Space maintainers require follow-up. Parents/guardians should be informed of the need to immediately notify the practice if the space maintainer becomes loose, is dislodged from the tooth, broken, or is interfering with the eruption of a permanent tooth (Figure 16.2). If the primary molar banded for the appliance exfoliates, a second appliance may be indicated to maintain space for a second premolar. Fixed appliances may increase the incidence of caries on the banded molar or adjacent teeth in children with high-caries risk (Fricker et al., 2008). Poor oral hygiene can result in decalcification at the cervical margin of the band. Cementing bands with glass ionomer cement may reduce the risk of decalcification and caries. Removing the appliance to perform prophylaxis may be advisable every 6 months. A portion of the appliance may impinge on the gingival tissues after a period. Any complaint of discomfort by the child should be reported to the practice. Documentation in the patient’s chart of provision of this information to parents is advisable. Mean survival times for space maintainers are reported as between 26 and 27 months. The main reasons for failure were cement loss, split bands, eruption interference, bent wire, and solder breakage (Fathian et al., 2007). A lingual arch wire with a long arm has a significantly higher chance of solder breakage. Some insurance companies provide a code to recement an appliance.
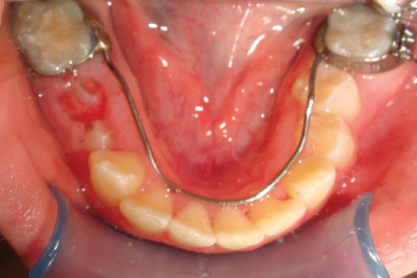
Figure 16.2 Lingual arch wire interfering with eruption of mandibular second premolar.
Primary incisors
After eruption of the primary canines, premature loss of one or more primary incisors due to trauma or caries results in negligible space loss (Fricker et al., 2008). Space maintenance is necessary only for aesthetic concerns or parental desire (Simon et al., 2012; Kupietzky, 2001). If a digit-sucking habit is of enough intensity, the space for the erupting permanent incisor may be reduced (American Academy of Pediatric Dentistry, 2014a). With significant overjet due to a parafunctional habit, fabrication of a partial denture (pedo partial) should be delayed until cessation of the habit. A fixed partial denture can be fabricated for both the maxilla and mandible with one or more denture teeth (Figure 16.3). If primary molar bands are not available when the impression is obtained or if the child cannot cooperate for banding, banding can be performed on the plaster model by the laboratory fabricating the appliance.

Figure 16.3 Maxillary and mandibular pedo partials for premature loss of primary incisors.
First primary molar
If the maxillary or mandibular first permanent molars are fully erupted and in good occlusion, and if the permanent incisors are erupted, space maintenance may not be necessary. In addition, if the child is younger than 4 years, and a periapical radiograph shows the first permanent molar to be a few millimeters below the alveolar bone or with less than one-half root formation, placement of a space maintainer may be delayed until closer to the anticipated time of eruption of the first permanent molar.
With loss of the first primary molar, before the eruption of the first permanent molar or when the first permanent molar is erupting, a band and loop in the maxilla or mandible or lingual archwire in the mandible is necessary to avoid mesial drift of the second primary molar into the extraction site (Tunison et al., 2008). For premature loss of a first primary molar in the maxilla or mandible, the second primary molar is banded, and the loop extends mesially to the distal of the primary canine (Figures 16.4 and 16.5).

Figure 16.4 Band and loop for premature loss of maxillary first primary molar with unerupted first permanent molar.

Figure 16.5 Band and loop for premature loss of mandibular first primary molar with partially erupted first permanent molar.
Although a first permanent molar may be fully erupted in the maxilla, space loss has been shown to occur primarily as a result of distal drift of the primary canine into the extraction site and palatal movement of the maxillary incisors (Figure 16.6) (Lin et al
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


