Chapter 17
Pulpal treatment in young permanent incisors following traumatic injuries
Joe H. Camp
Pulp capping and pulpotomy
Preservation of vitality in young permanent immature teeth is imperative to allow completion of root formation in order to have the strongest root possible. If injury occurs resulting in pulpal necrosis before dentinogenesis is completed, retention of the tooth is compromised by diminished root length and thinness of dentin. The thinner dentinal walls of the root lead to increased root fracture. The decrease in root length results in less root-to-crown ratio and may lead to tooth mobility with resultant loss of attachment apparatus.
In a 4-year study, Cvek (1992) reported significant increase in cervical root fracture in endodontically treated immature teeth. Dependent on the stage of development, fractures ranged from 77% in teeth with the least root development to 28% with the most developed roots (Figures 17.1 and 17.2).
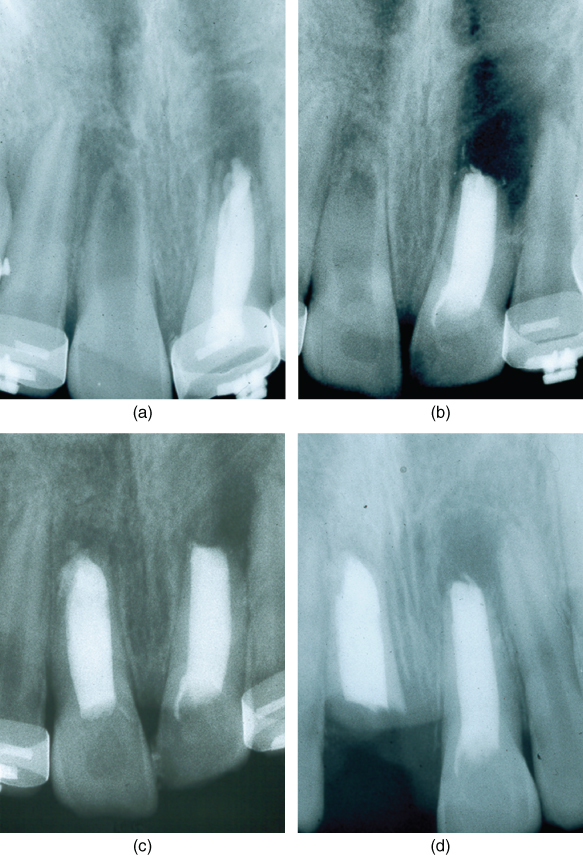
Figure 17.1 Fractured root of the maxillary right central incisor following successful apexification with calcium hydroxide and filling of root canal with guttapercha. (a) Preoperative radiograph. Unsuccessful previous root canal treatment with guttapercha in the left central incisor. (b) Successful apexification of the right incisor. The left incisor has root canal filled with guttapercha followed by an apical curettage. (c) Radiograph at 18 months. The right central has been filled with guttapercha. The lesion at the apex of the left incisor is healing. (d) Fracture of the thin root of the right central incisor 3 months later. The left incisor continues to heal apically.
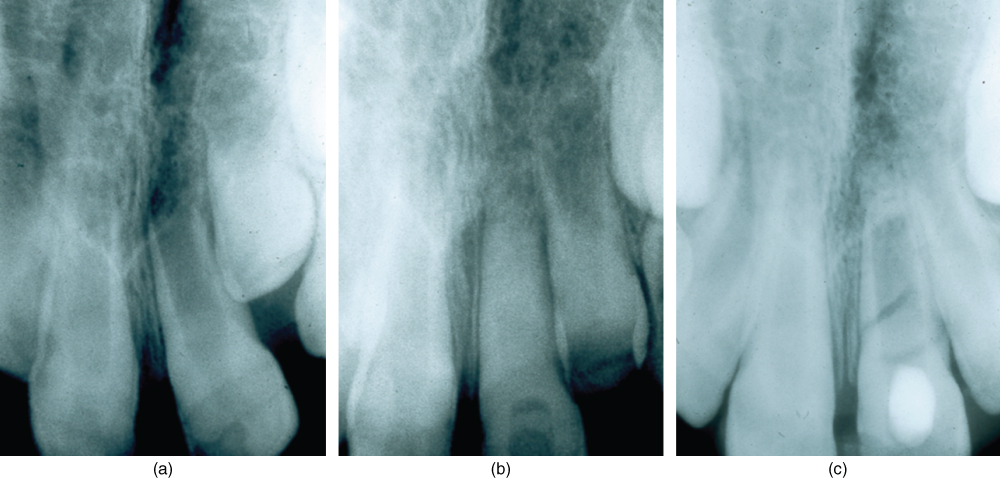
Figure 17.2 Root fracture of maxillary left central incisor while undergoing apexification with calcium hydroxide. (a) Preoperative radiograph of left central incisor with necrotic pulp and incompletely formed root. (b) Canal cleansed and filled with calcium hydroxide. (c) 18-month radiograph. Apexification completed but before the canal is sealed with guttapercha, another injury results in root fracture and the tooth must be extracted.
Direct pulp capping (Figure 17.3) and pulpotomy attempt to preserve pulpal vitality by the application of a medicament or dental material to the exposed pulp. Pulpotomy differs from pulp capping only in that additional pulp tissue is removed before placement of the pulp-capping agent. The success rates of these procedures following injury in the young teeth are highly successful (Cvek and Lundberg, 1983; Fuks et al., 1987). While there is much disagreement on these vital procedures versus pulpectomy and root canal filling, there is almost universal agreement these procedures are indicated in teeth with immature apices.
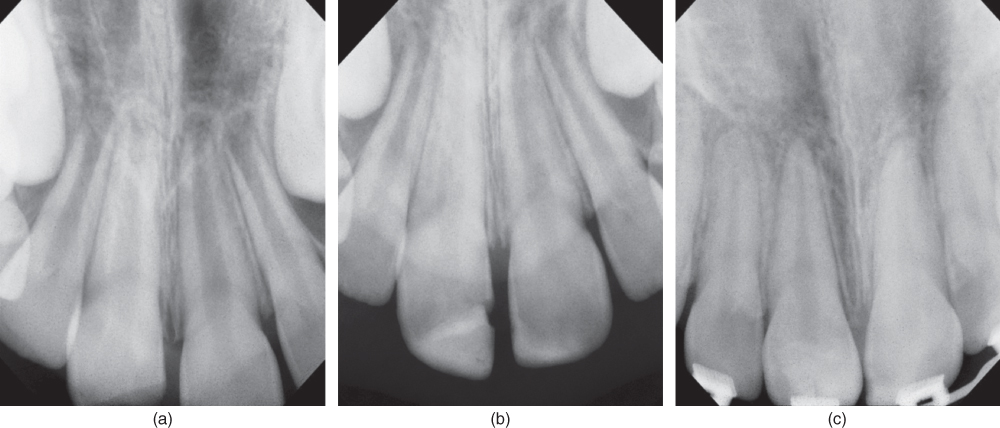
Figure 17.3 Apical closure and root completion following direct pulp capping in maxillary right central incisor. (a) Radiograph of fractured left incisor with pulp exposure. Note the immature roots. (b) Radiograph of MTA pulp capping covered with composite resin. (c) Radiograph 4.5 years after pulp capping showing dentinal bridging and completed root formation.
In young fractured teeth with pulp exposure, Cvek (1978) and Cvek and Lundberg (1983) have shown that inflammation and/or infection will be confined to the surface 2–3 mm. The underlying tissue will respond favorably to pulpotomy. Neither the exposure size nor time between injury and treatment up to 90 days is critical for healing when only the superficial layers of pulp are removed. It is usually not necessary or desirable to remove all the coronal pulp tissue. This partial pulpotomy is commonly referred to as a Cvek pulpotomy (Cvek, 1993) (Figures 17.4 and 17.5).
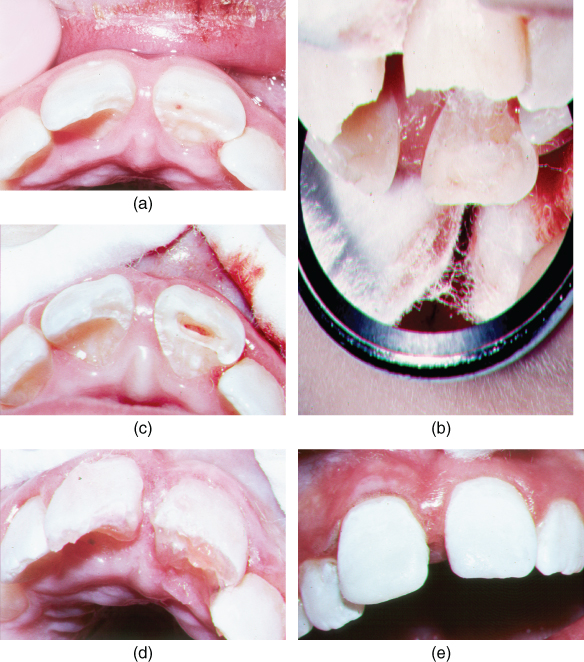
Figure 17.4 Cvek pulpotomy with MTA on a maxillary right central incisor. (a) Clinical appearance of pup exposure 4 days after injury. The right incisor has a pulp exposure and the left incisor has a minor dentin fracture. (b) Three millimeters of the pulp has been removed with a clean amputation, washed, and a wetted cotton pellet placed against the pulp to control hemorrhage. (c) The amputation site after cotton is removed. Note the lack of hemorrhage. (d) The pulp has been capped with 1.5 mm of white MTA. A thin layer of light-cured composite has been placed over the MTA and cured to protect it during sealing of the tooth. (e) The two central incisors are etched. (f) Sealing of the incisors with bonded composite restorations. A definitive well-contoured restoration will be placed in 8 weeks after healing has occurred.
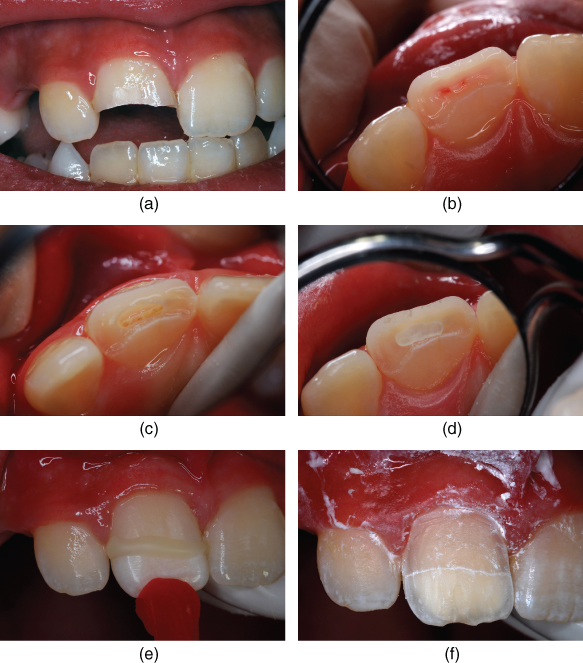
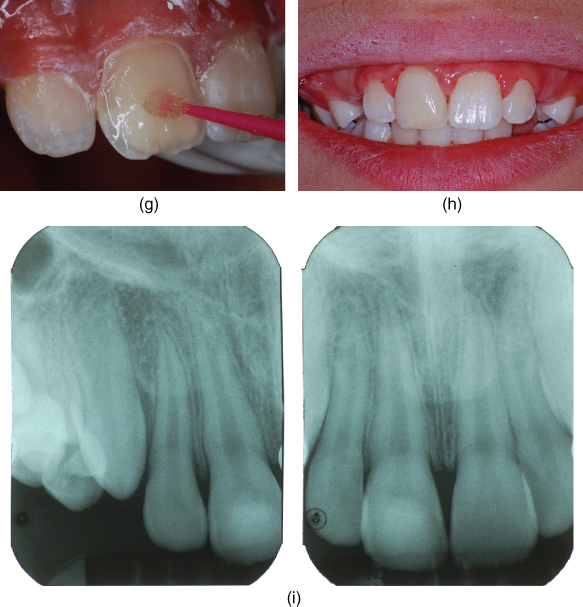
Figure 17.5 Cvek pulpotomy with Ca(OH)2 and restoration of crown on traumatically injured maxillary central incisor. (a) Facial views of fractured incisor (courtesy of Dr. Ted Croll). (b) Incisal view of tooth revealing pulp exposure (courtesy of Dr. Ted Croll). (c) Pulp chamber after 2 mm diamond bur preparation and hemostasis (courtesy of Dr. Ted Croll). (d) Ca(OH)2 placed in prepared chamber (courtesy of Dr. Ted Croll). (e) Fractured coronal segment reattached with resin-modified glass-ionomer cement (courtesy of Dr. Ted Croll). (f) Facial enamel preparation for placement of direct bonded resin-based composite veneer. (g) Self-etching resin bonding agent applied (courtesy of Dr. Ted Croll). (h) Restored tooth 26 months immediately following routine prophylaxis (courtesy of Dr. Ted Croll). (i) Two radiographic views of 26 month after Cvek pulpotomy (courtesy of Dr. Ted Croll).
Many medicaments and materials have been used for pulp capping and pulpotomy. Traditionally, calcium hydroxide Ca(OH)2 has been the most widely used agent of choice (Figure 17.7). However, additional recent research has shown mineral trioxide aggregate (MTA) to be more biologic while producing better results (Abedi et al., 1996; Pitt Ford et al., 1996). MTA has become the agent of choice (Figures 17.6 and 17.7).
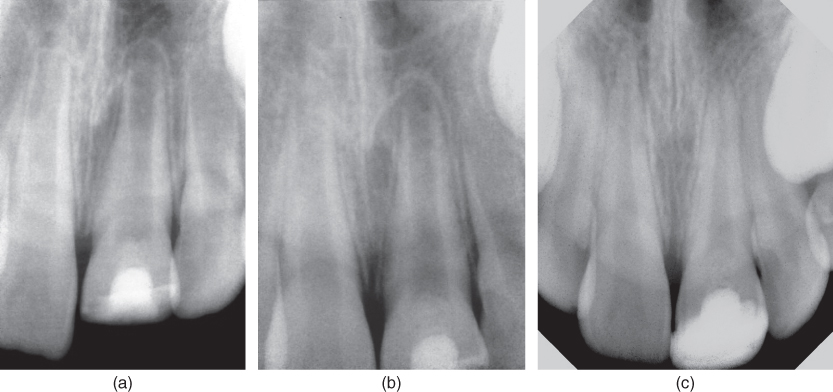
Figure 17.6 Cvek pulpotomy with MTA on a maxillary left central incisor with an open apex. (a) Radiograph 3 months after pulpotomy. Note the dentin bridge. (b) Radiograph 6 months after pulpotomy. The dentin bridge has thickened. (c) Radiograph 3.5 years after Cvek pulpotomy. The root formation is completed and the apex closed. The dentin bridge has thickened but the root is free of abnormal calcification.
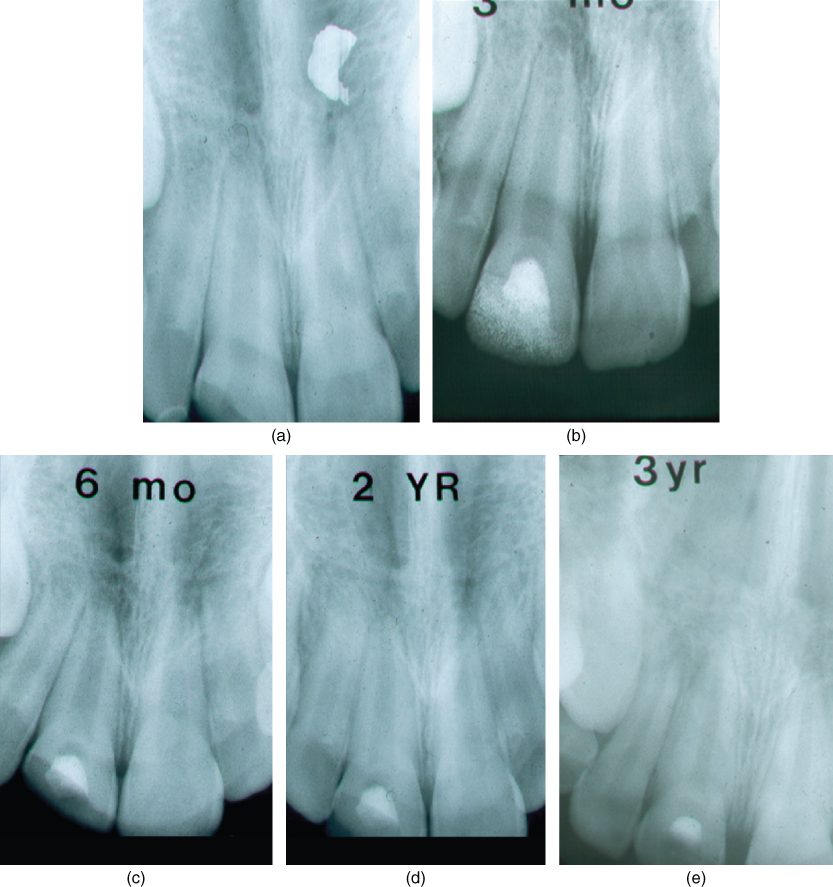
Figure 17.7 Cvek pulpotomy with calcium hydroxide on a maxillary right central incisor with an open apex. (a) Preoperative radiograph of fractured incisor with pulp exposure. (b) Radiograph at 12 weeks showing dentin bridge. (c) Radiograph at 6 months. Note the dentin bridge has not thickened any further. (d) Radiograph at 2 years. Root formation is completed. (e) Radiograph at 3 years. The canal is not calcified.
Healing is directly related to the capacity of the capping agent and restoration to provide a biologic seal against bacterial leakage while simultaneously forming a dentinal bridge. MTA provides a biologically active substrate to which cells are attached. Calcium released from the MTA reacts with phosphate in the tissue fluid to produce hydroxyapatite (Sarkar et al., 2002).
In the Cvek pulpotomy, only tissue judged to be inflamed is removed. Removal of tissue is accomplished with an abrasive diamond or round carbide bur using high-speed and copious water spray. All fibers of the pulp coronal to the amputation must be removed, otherwise hemorrhage will persist. After tissue removal is completed, the site is washed with sterile water or saline to remove all debris. Blowing air on the pulp is contraindicated because it will cause damage to the tissue from desiccation.
Hemorrhage control is obtained by light pressure on the pulp with a dampened cotton pellet. Hemostasis should be achieved in 1–2 min (Figures 17.4b, 17.4c and 17.5
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


