
Therefore the communication of form is by shadow. A comparison of Figures 2-1 and 2-2 makes this concept apparent. Dental restorations can mimic the shadows of adjacent teeth to create a shape that blends with the surrounding tooth forms. Shadow manipulation can make poorly shaped teeth esthetically pleasing.
The principles of color
In 1666, Sir Isaac Newton observed that white light passing through a prism divided into an orderly pattern of colors now termed the spectrum. He also discovered that these colors produced white light when passed back through the prism, proving that all spectral colors were in the original beam.1
Color, as the eye interprets it, is either a result of absorption or reflection. In absorption, a white light is passed through a filter. The colors that pass through the filter and reach the eye are perceived as the color of the filter. In reflection, as with solid objects, the perceived color is the portion of the spectrum that is reflected back to the eye.
Light entering the eye stimulates the photoreceptor rods and cones in the retina. The energy is converted through a photochemical reaction into nerve impulses and carried through the optic nerve into the occipital lobe of the cerebral cortex. The rod cells are responsible for interpreting brightness differences and value. The cone cells function in hue and chroma interpretation. If the light source contains all the colors of the spectrum, a true reading occurs. If the light source is deficient in a certain color, a false reading occurs (see the section on Metamerism). Precise description of these colors and organization of their interrelationships, however, did not occur until 249 years after Newton’s work. Robert Louis Stevenson, one of the most concise writers in the English language, demonstrated the problems of describing color: “red—it’s not Turkish and it’s not Roman and it’s not Indian, but it seems to partake of the two last.”2 In 1915, Albert Henry Munsell created an orderly numeric system of color description that is still the standard today. In this system color is divided into three parameters—hue, chroma, and value.3
Hue
Hue (Fig. 2-3) is the name of the color. Roy G. Biv ( R ed, O range, Y ellow, G reen, B lue, I ndigo, V iolet) is an acronym for the hues of the spectrum. In the younger permanent dentition, hue tends to be similar throughout the mouth. With aging, variations in hue often occur because of intrinsic and extrinsic staining from restorative materials, foods, beverages, smoking, and other influences.

Chroma
Chroma (Fig. 2-4) is the saturation or intensity of hue; therefore it can only be present with hue. For example, to increase the chroma of a porcelain restoration, more of that hue is added. Chroma is the quality of hue that is most amenable to decrease by bleaching. Almost all hues are amenable to chroma reduction in vital and nonvital bleaching.4 In general, the chroma of teeth increases with age.

Value
Value (Fig. 2-5) is the relative lightness or darkness of a color. A light tooth has a high value; a dark tooth has a low value. It is not the quantity of the “color” gray, but rather the quality of brightness on a gray scale.5 That is, the shade of color (hue plus chroma) either seems light and bright or dark and dim. It is helpful to regard value in this way because the use of value in restorative dentistry does not involve adding gray but rather manipulating colors to increase or decrease amounts of grayness.

Color (HUE) relationship
The color wheel
Hues, as used in dentistry, have a relationship to one another that can be demonstrated on a color wheel. The relationships of primary, secondary, and complementary hues are graphically depicted by the color wheel (Fig. 2-6).
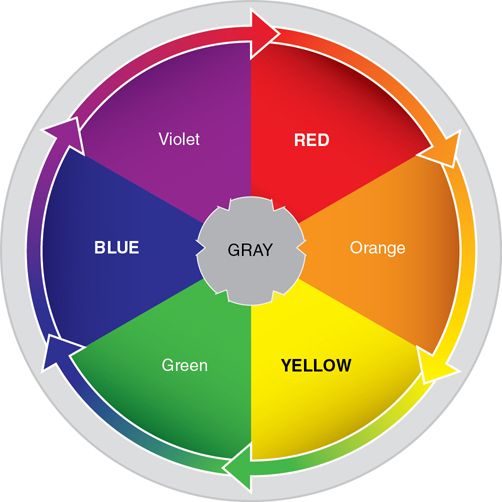
Primary hues
The primary hues—red, yellow, and blue—form the basis of the dental color system. In dentistry, the metal oxide pigments used in coloring porcelains are limited in forming certain reds; therefore pink is substituted. The primary hues and their relationships to one another form the basic structure of the color wheel.
Secondary hues
The mixture of any two primary hues forms a secondary hue. When red and blue are mixed they create violet, blue and yellow create green, and yellow and red create orange. Altering the chroma of the primary hues in a mixture changes the hue of the secondary hue produced. Primary and secondary hues can be organized on the color wheel with secondary hues positioned between primary hues.
Complementary hues
Colors directly opposite each other on the color wheel are termed complementary hues. A peculiarity of this system is that a primary hue is always opposite a secondary hue and vice versa. When a primary hue is mixed with a complementary secondary hue, the effect is to “cancel” out both colors and produce gray. This is the most important relationship in dental color manipulation.
When a portion of a crown is too yellow, lightly washing with violet (the complementary hue of yellow) produces an area that is no longer yellow. The yellow color is canceled out and the area will have an increased grayness (a lower value). This is especially useful if the body color of a crown has been brought too far incisally and if a more incisal color is desired toward the cervical area. If a cervical area is too yellow and a brown color is desired, washing the area with violet cancels the yellow. This is followed by the application of the desired color, in this situation brown.
Complementary hues also exhibit the useful phenomenon of intensification. When complementary hues are placed next to one another, they are each intensified and appear to have a higher chroma. A light orange line on the incisal edge intensifies the blue of an incisal color.
Hue sensitivity
After 5 seconds of staring at a tooth or shade guide, the human eye accommodates and becomes biased. If an individual stares at any color for longer than 5 seconds and then stares at a white surface or closes his or her eyes, the image appears, but in the complementary hue. This phenomenon, known as hue sensitivity, adversely affects shade selection.
Metamerism
Metamerism is a phenomenon that can cause two color samples to appear as the same hue under one light source, but as dissimilar hues under a different light source.
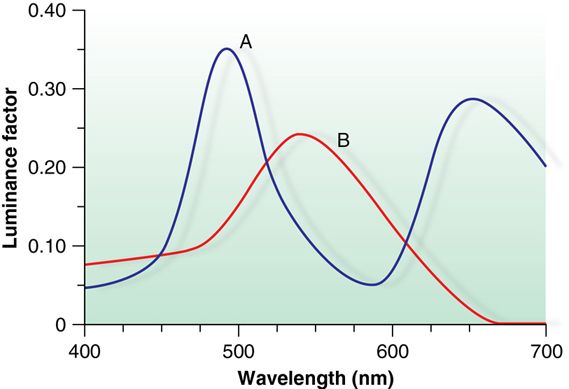
There is more than one way to produce a color. It can either be pure, or a mixture of two other colors (e.g., pure green versus a mix of blue and yellow). Pure green reflects light in the green band, but the green mixture reflects light in the blue and yellow bands simultaneously. If both colors are exposed to a light with a full color spectrum, they will appear similar. If, however, they are exposed to a light source that does not contain light in the blue band, the two colors will appear dissimilar. True green will still appear green, but the mixture will appear yellow because without a source of light in the blue band the blue component of the mix is not visible.
A spectral curve is a measure of the wavelength of light reflected from a surface. It reveals the actual component colors reflected from an object (Fig. 2-7).5
Clinical relevance.
Metamerism complicates the color matching of restorations. A shade button may match under incandescent lighting from the dental operatory lamp but not under fluorescent lighting in the patient’s workplace.
A color selection that works well under a variety of lights is preferred to a match that is exact under one source of light but completely wrong under others.6 Usually three sources of light are available in the dental operatory:
Color-corrected fluorescent lamps more closely approximate natural daylight and some practitioners prefer them as the standard in dental operatories. If the entire office is illuminated by color-corrected fluorescent lamp, one room should have cool white fluorescent lighting for comparative shade matching. The color match that appears best in these three lights is usually preferable.
Opacity
An opaque material does not permit any light to pass through. It reflects all the light that is directed onto it.
Clinical relevance.
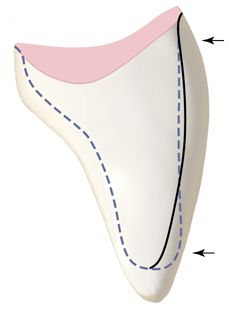
A porcelain-fused-to-metal restoration must have a layer of opaque porcelain applied to the metal substructure to prevent the color of the metal from appearing through the translucent body and incisal porcelains. Improper tooth reduction results in two unacceptable results:
1. An ideally contoured restoration with minimal porcelain thickness and too much opaque porcelain, resulting in a “chalky” appearance
2. A bulky, poorly contoured restoration with ideal porcelain thickness
Tooth reduction must be sufficient to allow enough room for an adequate bulk of porcelain (Fig. 2-8).
Translucency
Translucent materials allow some light to pass through them. Only some of the light is absorbed. Translucency provides realism to a dental restoration.
Depth
In restorative dentistry, depth is a spatial concept of color blending combining the concepts of opacity and translucency. In the natural dentition, light passes through the translucent enamel and is reflected out from the depths of the relatively opaque dentin.
White porcelain colorants used in color modification are opaque. Gray porcelain colorants are a mixture of black and white. A tooth restoration with a white opaque colorant on the surface appears artificial because it lacks the quality of depth that would be seen if the opaque layer were placed beneath a translucent layer of porcelain. Similarly a bright restoration (high value) in need of graying (a decrease in value) would appear falsely opaque if it were simply painted gray. Adding a complementary hue, however, both decreases the value and adds to the translucency. If characterization is added to porcelain to represent white hypoplastic spots or gray amalgam stains, white or gray colorant can be used, but translucency will be reduced in these areas.
Depth may be problematic if translucent composite resins are used to restore Class III or IV cavities that extend completely from facial to lingual surfaces. The restoration may appear gray or overly translucent. However, if a more opaque composite resin is placed on the lingual portion of the restoration and then overlaid with a translucent resin, a natural illusion of depth results.
Shade progression.
The maxillary anterior teeth and premolars are not uniform in shade.7 The lateral incisors are similar in hue to the central incisors but are slightly lower in value. The canines are also lower in value than the incisors but also exhibit greater chroma saturation. The premolars have values similar to the lateral incisors.7
Fluorescence
Fluorescence occurs when a material absorbs short wavelength light (usually near ultraviolet) and reemits light of longer wavelength (usually visible light).8 Because of its higher organic content, dentin is the primary source of fluorescence in human teeth. Fluorescence reduces chroma and raises value without effecting translucency.9 Fluorescent porcelains mimic dentin resulting in brighter and more vital, life-like restorations.8
Opalescence
Opalescence occurs when a material appears as one color when light is reflected off its surface and a different color when light is transmitted through it.10 Opalescence mimics enamel and is highly wavelength dependent. Opalescent materials such as hydroxyapatite act like a prism and tend to refract shorter wavelengths (violet) more than longer wavelengths (red and yellow).6 Therefore, enamel will transilluminate red and yellow light but scatter violet and blue light within its body. This has the effect of causing the incisal enamel to appear bluish (and translucent) as well as producing optical depth.11
Bleached teeth.
Tooth bleaching dehydrates enamel and sometimes dentin, and sometimes removes pigmented organic material from between the hydroxyapatite crystals. Bleaching changes the hue, chroma, and value of a tooth, resulting in a brighter appearance.12 Whitening resulting from dehydration is temporary and reverses upon tooth rehydration. Removal of pigment, if it occurs at all, is permanent, although restaining may occur in the future. The degree of “rebound” shortly following bleaching depends on the amount of dehydration and subsequent rehydration that occurs. After bleaching, shade matching should be delayed for at least 1 month.8
The principles of form
Perception
Unconscious perceptions about color, size, shape, age, and gender are based on certain natural biases indigenous to an individual’s cultural background. Perceptual biases can be divided into two types: cultural and artistic.
Cultural biases
Cultural biases are naturally occurring environmental observations about the world.. We perceive (and believe) that darker, heavily worn, highly stained, longer teeth belong to an older person because we know that teeth naturally darken, wear, and stain in grooves and along the cervical area with age, and that they lengthen because of gingival recession. We perceive (and believe) rounded, smooth-flowing forms are feminine, whereas harsher, more angular forms are masculine.
Masculine and feminine.
Culturally defined masculine qualities may enhance the appearance of a woman. (Many feminine fashions include a modification of a shirt and tie.) However, usually these masculine nuances appear best on a woman with stereotypically feminine features. Square, angular anterior teeth, therefore, may be desirable on what some might term a a more “feminine” woman, but on other women this tooth shape may not be as flattering. In Western culture, contrast evokes a certain allure. With no contrast, the allure is gone.
The golden proportion.
Western civilization has drawn the conclusion that for objects to be proportional to one another the ratio of 1:1.618 is esthetically pleasing. Much has been hypothesized from this ratio, from the mathematical relationship of the chambers of the nautilus shell to facial proportions. As a rule, if the apparent (see the section on The Law of the Face) size of each tooth, as observed from the frontal view, is 60% of the size of the tooth anterior to it, the relationship is considered esthetically pleasing. That is, if proportionately the apparent width of the central incisor is 1.608, the lateral incisor and canine should be 1.0 and 0.608, respectively.13 This “golden proportion” occurs in 80% of the population.14
Artistic biases
Artistic biases are inherent in the perception of form. The most important of these is the perception that light approaches and dark recedes; this is the principle of illumination. 15 The light areas in Figure 2-2 appear to be positioned forward, whereas the darker areas appear to recede. This produces the illusion of a third dimension (depth) despite the two-dimensional nature (length and width) of the printed page. This bias applies to clothing, cosmetics, and teeth. The purpose of cosmetic “makeup” is to enhance facial contours (Fig. 2-9).

The second artistic bias of great importance in dentistry is the use of horizontal and vertical lines. A horizontal line causes an object to appear wider, whereas a vertical line causes an object to appear longer (Fig. 2-10). This can be termed the principle of line.

These cultural and artistic biases are so entrenched in our subconscious thought that they are unavoidable and automatic. Artistic manipulation of these biases allows the esthetic dentist to fool the eye of the observer when fabricating artificial esthetic restorations.
Illusion
Illusion is the art of changing perception to cause an object to appear different than it actually is. Teeth can be made to appear wider, narrower, smaller, larger, shorter, longer, older, younger, masculine, or feminine. An understanding of the basic principles of perception and their use in controlling illusion must precede their use.
Computerized digital shade technology
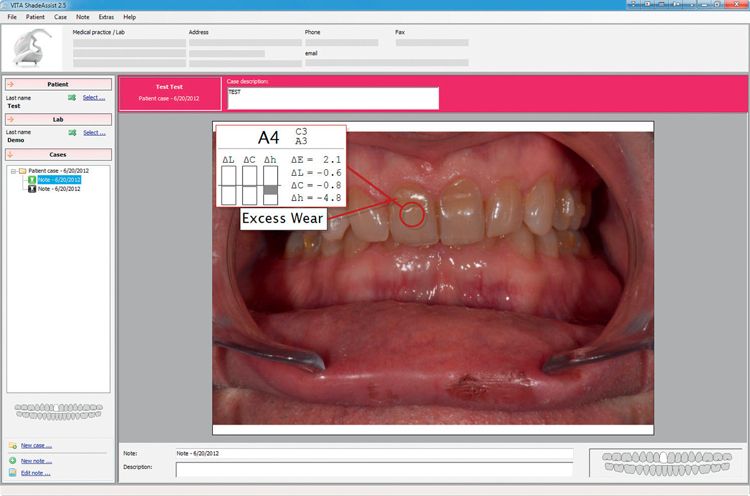
The electronic dental color-measuring device has recently been introduced into the dental armamentarium (e.g., VITA Easyshade Compact, Vident, Inc., Fig. 2-11). These devices use a digital spectrophotometer that measures the spectral reflectance or spectral transmittance of a specimen.16 White light from a tungsten-filament bulb is dispersed by the spectrophotometer into a wavelength of between 5 and 20 nm,17 which is directed at a specimen. The amount of light reflected from the specimen is measured for each wavelength in the visible spectrum and is correlated to popular dental shade guides. Some devices include software (e.g., VITA ShadeAssist software, Vident, Inc.; Fig. 2-12) that can read and record the information measured by the device.
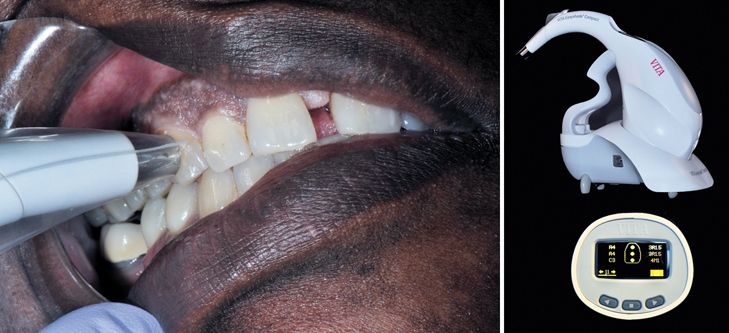
They are unaffected by metamerism and have shown great reproducibility and accuracy. 17–20 Because the cost of these instruments inevitably decrease over time, they may become commonplace in clinical dental shade management.
Using the principles of perception to control illusion
Principle of illumination
The principle of illumination can be manipulated by the dentist to change the apparent size and shape of a tooth through illusion. This bias is the key to The Law of the Face.
The law of the face
The law of the face is the most important single concept in shaping dental restorations. Understanding this concept and its interplay with the concept of light and dark enables the esthetic dentist to shape all esthetic restorations correctly.
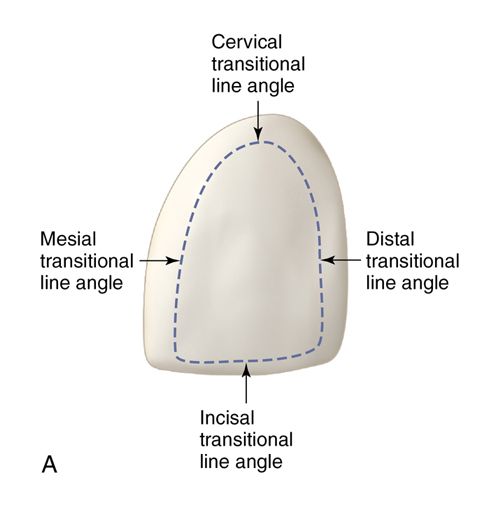
The face of a tooth is the area on the facial surface of anterior and posterior teeth that is bounded by the transitional line angles as viewed from the facial (buccal) aspect (Fig. 2-13A). The transitional line angles mark the transition from the facial surface to the mesial, cervical, distal, and incisal surfaces. The tooth surface slopes lingually toward the mesial and distal approximating surfaces and toward the cervical root surface from these line angles. Often no transitional line angle appears on the incisal portion of the facial surface; in this situation, the face is bounded by the incisal edge or the occlusal tip. Shadows created as light strikes the facial surface of the tooth begin at the transitional line angles. These shadows delineate the boundaries of the face.




Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


