Chapter 8
Extraction of primary dentition
Jane A. Soxman
A periapical radiograph to evaluate the location, presence, or absence of the permanent successor and informed consent should be obtained before extraction. The length of unresorbed roots after a primary tooth’s extraction may surprise the parent/guardian. The use of the pre-extraction radiograph and/or the use of a mixed dentition typodont (Kilgore International) are good methods to show root length before an extraction (Figure 8.1).

Figure 8.1 Mixed dentition typodont to show root length of primary dentition.
Curette
After administration of local anesthesia, a sterile curette may be used to sever the gingival attachment (Figure 8.2). This first step of the procedure may predict the behavior for the remainder of the procedure, as a very anxious child will respond negatively to even slight pressure with the curette. Anxiety is the biggest predictor of poor pain control (Nakai et al., 2000).

Figure 8.2 Curette severing the gingival attachment.
Luxation
Luxation (loosening) is the most important step to facilitate extraction and avoid root fracture of a primary molar. The interproximal contacts of primary molars are broad, flat and without cervical constriction. The tip of the instrument for luxation should be narrow enough to be placed through the embrasures of the primary molars (Figure 8.3a and 8.3b). This step may not be necessary for primary incisors and canines with conical, single roots but may be helpful in some cases. Primary incisors may be luxated using straight forceps with a labiolingual movement. During luxation, use caution not to include adjacent teeth, causing mobility. If an adjacent tooth is mobile before the extraction, the parent/guardian should be informed of the possibility of an unintentional extraction.
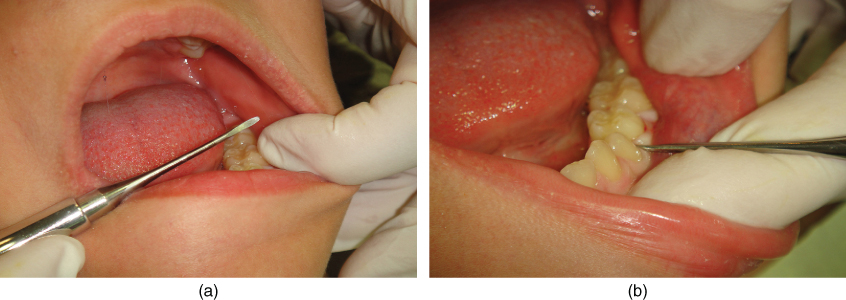
Figure 8.3 (a) Luxation instrument. (b) Luxation of primary molar.
The feeling of pressure during the luxation and extraction should be explained. Pushing on the child’s shoulder may demonstrate this sensation. If a previously cooperative child begins to cry, exhibiting pain during luxation, administration of additional local anesthesia is indicated. Injections through the mesial and distal papilla from buccal to lingual, along with injection into the gingival sulcus, are very effective. Palatal injection using the DentalVibe significantly reduces injection discomfort (Figures 8.4a, 8.4b, 8.4c, and 8.5).
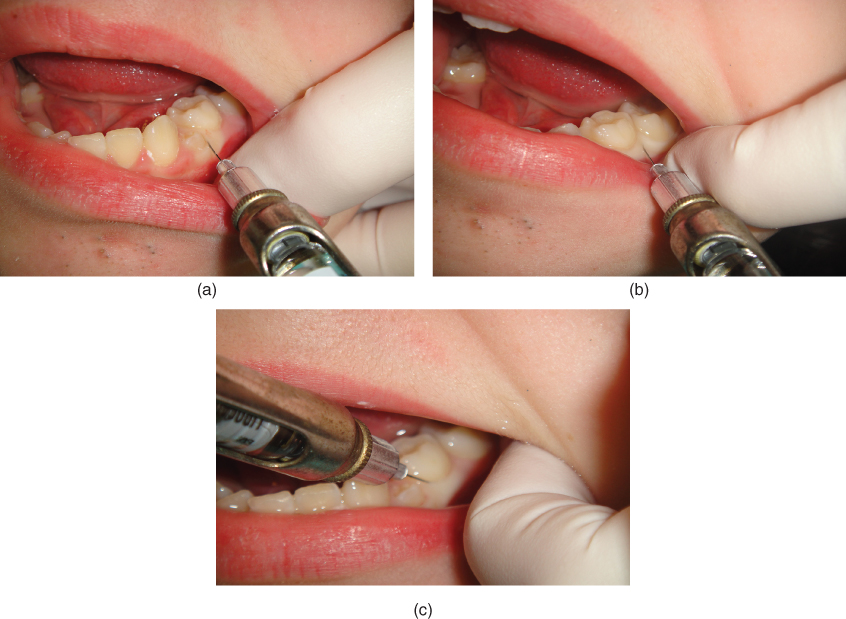
Figure 8.4 (a) Injection in mesial papilla. (b) Injection in distal papilla. (c) Injection into sulcus.

Figure 8.5 Palatal injection with DentalVibe.
Extraction
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


