Direct Posterior Restorations
The composition of composites has already been discussed in detail. This section outlines the step-by-step procedure for placing a direct posterior composite filling. Placing a direct posterior composite is quite demanding and to optimize the clinical success basic knowledge of the material and its behavior is a prerequisite.
The composites used in dentistry are very complex materials as far as their chemistry and behavior are concerned. According to their chemical composition, they should not be more biocompatible than other generally used restorative materials. It is especially important to realize this considering the fact that during the past few years the fear regarding the potential dangers of mercury being released from dental amalgams has increased.
282 Direct composite restoration in the posterior region
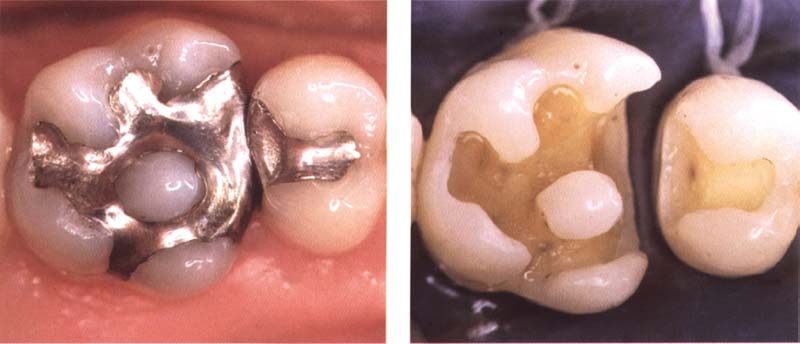
Left: Initial condition includes two amalgam restorations that are to be replaced. The indication for replacing existing amalgam restorations must carefully be judged by each dentist (e.g., caries) because the risk of secondary caries under composites is considerably higher than under amalgams.
Right: When removing the old amalgam, mercury is released. A rubber dam offers optimum protection.
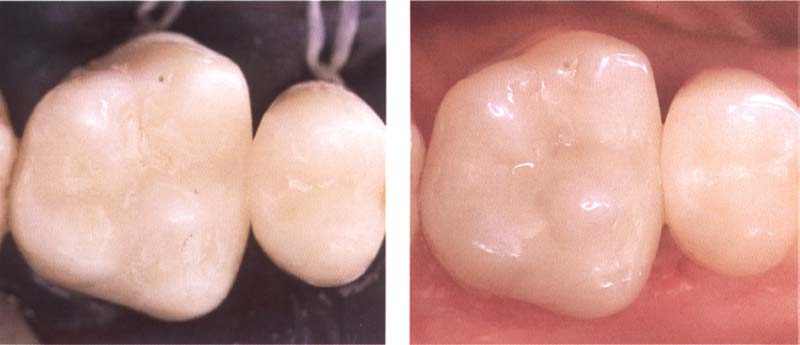
283 Finished restoration
Left: Rubber dam facilitates the placement of a direct composite restoration in the posterior region.
Right: Finished restoration.
Advantages and Disadvantages of Composites
Due to the fears surrounding amalgam, which have until now not been scientifically substantiated, some dentists have ceased using amalgam. Instead they are using composites to treat the posterior teeth. Considering the complex chemistry of composites and the rather limited knowledge we have gained regarding their interaction within the biological surroundings, this does not seem justified at the present time. In other words, the opinion that composites are more biocompatible than amalgam and gold has not been proved and should not be used as an indication to replace the amalgams.
If one looks at the available clinical results regarding composites, one can hardly claim that these materials are superior to the traditional restoration materials such as gold and amalgam. In actual fact, clinical studies indicate that the lifespan of composite restorations used for posterior teeth is inferior to that of amalgam and gold.
The inferior longevity can be attributed to the fact that composites are subject to more wear in vivo than metallic restorations, even if in vitro studies may refute this. However, there are many factors in the mouth that can not be imitated in vitro.
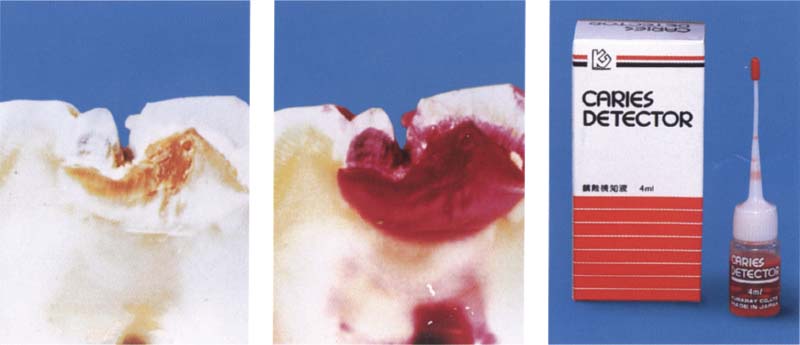
284 How the caries detector works
Left: An unstained carious lesion in cross section.
Middle: The caries detector stains only infected dentin.
Right: Caries detector by the Japanese company Kuraray (Osaka).
Courtesy of T. Yamada
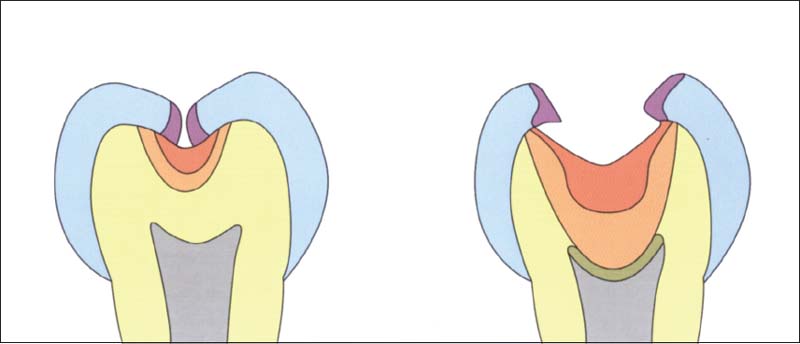
285 Structure of carious tooth in a schematic cross section
The caries detector stains only the outer, infected carious dentin (red). The dentist can focus on the diseased dentin layer and remove it virtually without pain. The dentin that is not stained by the caries detector, such as carious discolored inner dentin (orange) as well as the healthy dentin (yellow), will be left intact (green = secondary dentin).
(Adapted from T. Yamada et al. 1995.)
In addition, the risk of developing s/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


