Basic Principles of Aesthetic Dentistry
Aesthetic dentistry is a treatment concept that, in addition to the practical treatment of the defective tissue, includes recognizing the cause of disease needs and suitable treatment alternatives. The Swedish dentist Per Axelsson (1978) raised the following question: is there a difference in oral health between patients who visit the dentist twice a year and those who only visit the dentist when they experience pain? The result was astonishing: actually, it did not matter whether or not patients visited the dentist regularly because both patient groups lost their teeth. However, in the years following this study, Axelsson (1981) was able to show a crucial difference: patients who visit a dental practice with an established maintenance system can go through life with healthy teeth as long as they are willing to make regular follow-up visits after completing full-mouth rehabilitation.
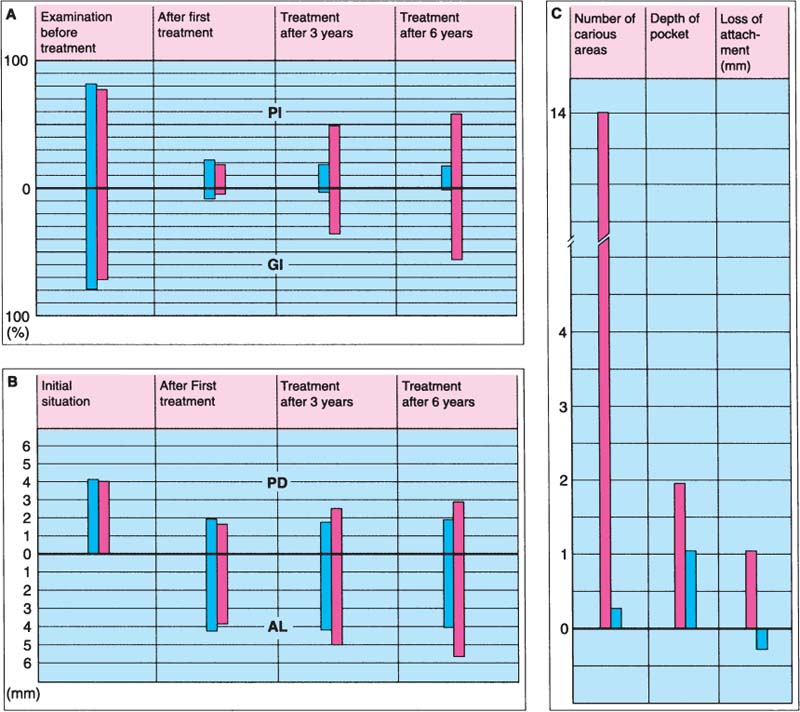
10 Importance of recalls
A Percentage of tooth surfaces covered with plaque (plaque index PI, upper half) and percentage of gingival units with inflammation (gingival index GI, lower half).
B Probing depth (PD) and attachment loss (AL).
C Carious surfaces, pocket depth, and attachment loss after 6 years.
 Recall group
Recall group
 Control group (not recalled)
Control group (not recalled)
Caries as an Infectious Disease and How It Can Be Prevented
It is not enough to simply restore an existing cavity. Caries is an infectious disease. If the infectious disease is not treated causally, there will be no lasting treatment success. This is especially important with tooth-colored restorations, restorations in the posterior teeth, and cemented restorations. Most resin cements, composite resin cements, and resin-modified glass ionomers have a relatively low filler content. Because of this they show somewhat inferior physical properties and with time the cement is washed away at the marginal area. As a result, the risk of caries will increase at this location.
The individual risk of caries and periodontitis of each patient should be established at the beginning of the treatment. Expensive, cemented, tooth-colored restorations should not be started until the initial therapy has been completed. In addition, it should be ensured before the treatment begins that the patient will regularly attend follow-up appointments.
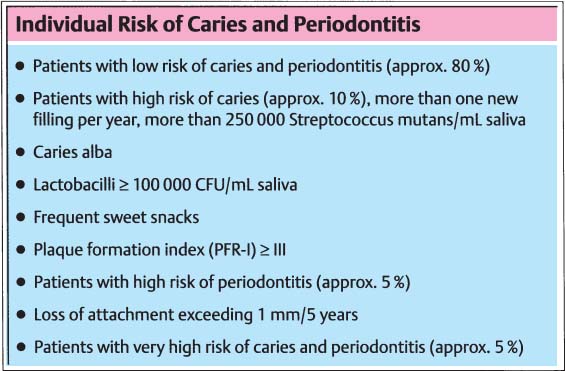
11 Summary
Before initiating aesthetic treatment, it is important to determine a patient’s caries and periodontitis risks. The factors listed on the right should be taken into consideration.
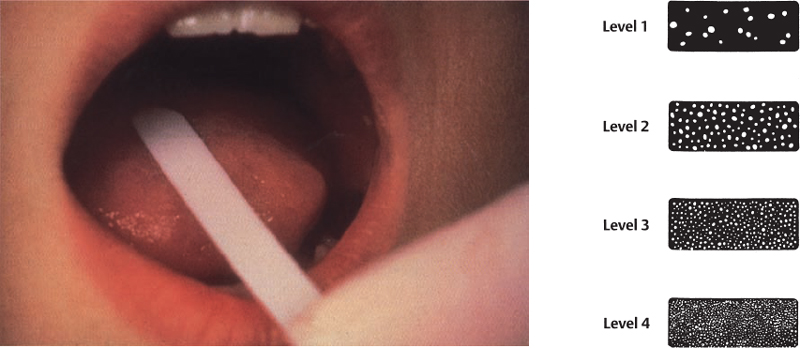
12 Microbiological examination of the oral cavity
To determine caries activity, the quantity of Lactobacillus or Streptococcus mutans can be readily determined using commercially available microbiological kits.
Right: Level 1 = low Lactobacillus activity; Level 4 = high caries risk due to high bacterial activity.
Left: Caries risk can easily be determined using a saliva sample.
In a dental practice, aesthetic dental medicine should be offered only in connection with a preventive dental concept based on the following four levels:
The goal of primary prevention is to secure healthy teeth and healthy periodontal tissues. Secondary prevention should prevent the recurrence of dental disease following therapy. The goal of tertiary prevention is to ensure that restorations and their restorative materials have preventive qualities. Therefore, cements that release fluoride and exhibit low solubility, such as glass ionomers, should be given preference to classic zinc phosphate cements.
Goals of Prevention
Two goals can be achieved with a well-designed preventive program:
1. In the age group below 19 years, interproximal restorations are not needed. In this age group, the use of sealants should have a high priority. If a posterior tooth requires a large restoration, the best possible material is selected after input from the patient. A small, initial carious lesion can be restored with a direct composite restoration, while a larger defect on a permanent molar can be restored with a gold restoration, based on longevity data available for these restorations. However, if instead the patient prefers a tooth-colored restoration (ceramic inlay/onlay or composite), those involved should be made aware of the increased risk of fracture and the related possibility of having to replace the restoration in the future.
Age groups with increased caries risk include 3, 7, and 8-year-olds and 13 to 15-year-olds. All teenagers undergoing orthodontic therapy belong to a very high risk group.
2. In the 20 to 50 year age group, the majority of patients should not develop any new carious lesions. Most restorations in this age group are replacements of existing fillings and crown restorations. The best possible restorative material should be selected in this case, too. It is important to select the best material to fit an existing defect rather than design a preparation to match a particular material. Ceramic restorations, particularly those fabricated using CAD/CAM technology (e.g., Cerec), force the preparation technique to be suited to the material, making the treatment less conservative. If it is a relatively small defect, the preferred materials include direct composites, gold alloys, or composite rather than ceramics.
The goal should be to save healthy tooth substance rather than to remove it for a particular restorative procedure.
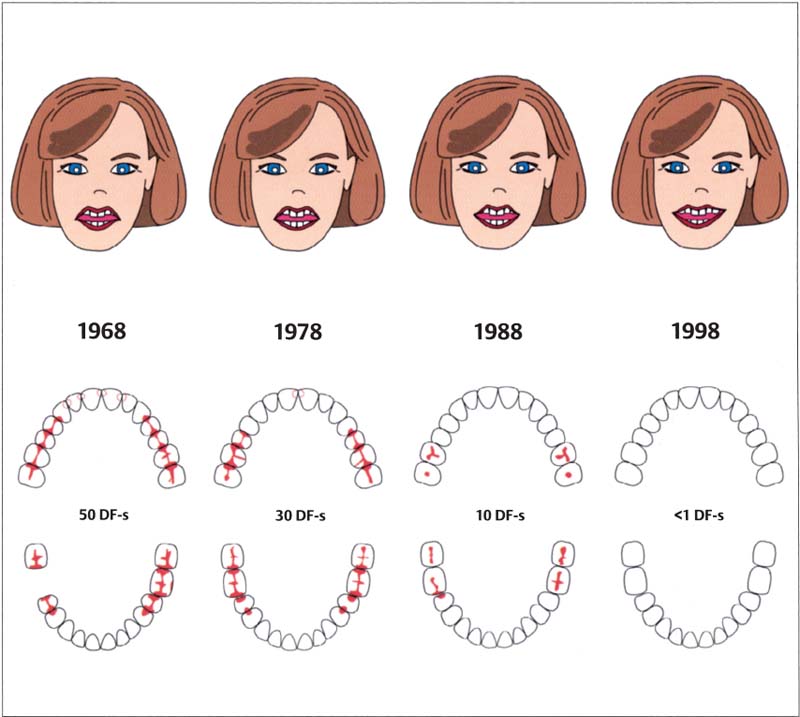
13 Reduction in caries lesions among adolescents in Karlstad, Sweden, over the past 30 years
Today, the majority of children will reach adulthood without suffering from caries. Incipient carious lesions can be treated with adhesive restorative materials.
Aesthetic Dentistry—A Treatment Concept
Aesthetic treatment, like any other dental treatment, consists of four phases:
Phase 1: Systemic Phase
This phase starts before the treatment begins. Its purpose is to protect both the therapist as well as the patient. Risk patients, for example patients with diabetes mellitus and cardiovascular or blood diseases, are identified before the actual treatment starts. This step includes consultations with the physician treating the patient.
Phase 2: Hygiene Phase
The goal of this phase is to establish a clean oral cavity to secure a healthy basis for the subsequent phase.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


