Electronic Dental Records and Decision Support Systems
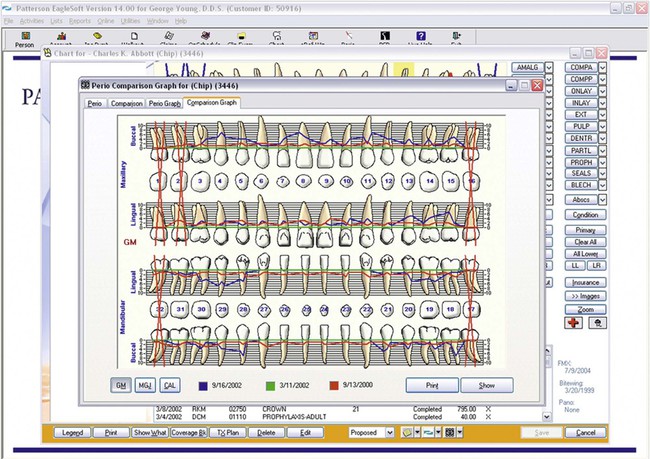
Dental practices are using electronic dental records (EDRs) for patient care to a significant and rapidly rising degree.14 While early on, computers primarily automated administrative and financial functions, they now increasingly support clinical patient documentation, digital radiographs, intraoral oral photos, and oral disease risk assessments. This shift in EDR use is generating vast amounts of patient data that could provide significant benefits to clinicians and researchers. Until now, clinicians have been able to track only individual patient outcomes through paper-based records. At the same time, researchers typically spend considerable time transcribing data from paper into electronic form to analyze data.
Functionalities and Components Available in Electronic Dental Records
Electronic Dental Record Use in Dental Practices
Over the last 20 years, the use of EDRs in dental practices has risen significantly worldwide, and especially in the United States.13,26 Early on, dental practices used computerized systems primarily for administrative functions, such as patient accounting and billing (94%), insurance processing (90.9%), and patient scheduling (83%).6 Only 37% of dental practices reported using a computer to maintain patient records at that time. Studies on EDR use in the England, Wales, and Sweden reported similar figures.28,26,19
More recent studies have pointed to a marked increase in EDR use for clinical documentation.14,13,6 In 2010, U.S. dental practices used EDRs to acquire and store radiographs (68%), intraoral photos and videos (67%), examination forms (54%), progress notes (54%), and dental charting (50%).6 Most practices maintained a hybrid system of patient records with some information spread across paper and the EDR. As opposed to 2% in 2006, in 2012 about 15% of practices maintained completely paperless records.14
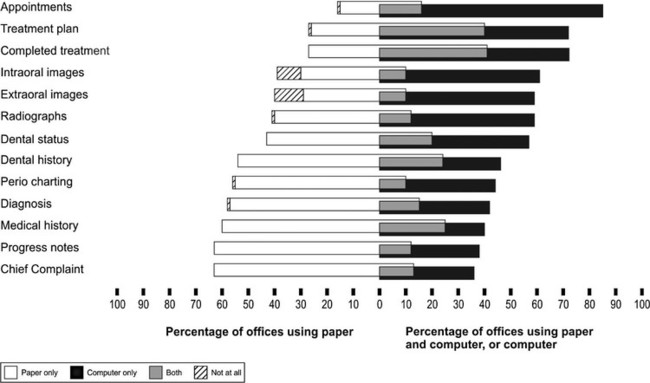
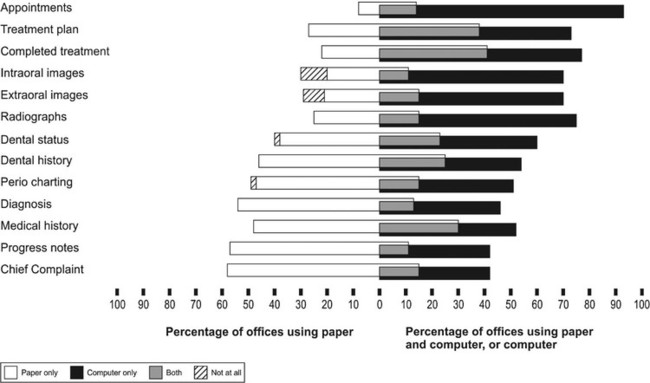
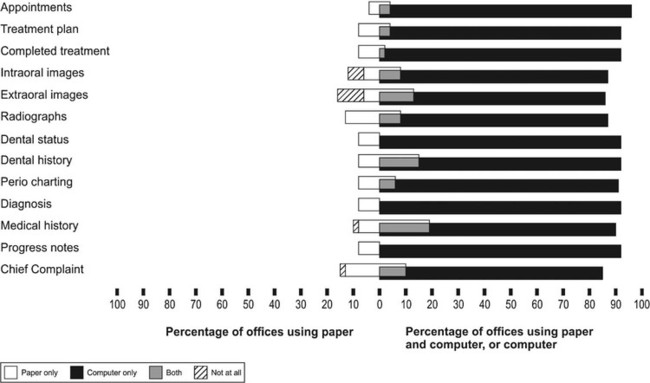
Figures 88-2, 88-3, and 88-4 illustrate how clinical information is stored in U.S. solo and group practices, as well as in Scandinavian group dental practices.14 These figures clearly show that more dental practices in Scandinavian countries stored clinical information on the computer than in the United States. Meanwhile, nearly all dental schools in the United States and Europe use (primarily commercial) EDR systems in some capacity.15,7 However, very few studies exist on how these systems are used in academic settings.
Commonly Used Electronic Dental Records
Four systems currently hold about 75% of the market in EDRs in the United States. They are Dentrix Dental Systems (Henry Schein; 37%), EagleSoft (Patterson Dental; 18%), and SoftDent and PracticeWorks (Carestream; 20%).14,13,6 About 100 other companies, most of them fairly small, develop and market EDR systems in the United States. Notable among them are the Windows-based MOGO, and Curve Dental and Dental Symphony, both web-based. While no general reports on EDRs commonly used in Europe exist, Al Dente (Nordenta, Horning, Denmark), Dental Suite (Plandent, Helsinki), and Opus (Planmeca, Helsinki) appear to dominate in Scandinavian countries.
Barriers to Using Electronic Dental Records
Limited Functionality for Communication and Collaboration.
Dental personnel collaborate extensively during patient care.9 However, existing EDRs provide limited support for collaboration and communication among dental team members. In addition, breakdowns related to technology interrupt the workflow, cause rework, and increase the number of steps in work processes.
Suboptimal Usability and Steep Learning Curve.
Several studies have reported poor usability of existing EDRs.* Two examples of usability problems are the separation of patient information across multiple screens, and the frequent mismatch between system design and task flow. As a result, users have to shift their attention from patients to EDRs to navigate through the information and to avoid making mistakes. Users believed they spent a longer time interacting with EDRs than with paper records, resulting in less face time with their patients.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


