8
The Relevance of Existing Dentures
This chapter makes the following key points:
- Existing dentures are often invaluable for diagnosis and treatment planning. For this a thorough assessment of the dentures, as described in Chapter 7, is essential. Most existing dentures, whether or not they have been worn successfully, can provide important information for all stages of treatment. Therefore they should be referred to regularly as treatment proceeds.
- Existing dentures are often very useful when carrying out certain treatment procedures.
- Most complete denture provision is concerned with the construction of replacement, rather than first dentures.
- The copy technique is an effective way of transferring design information accurately from existing to replacement dentures.
- As with most prosthetic treatments, good clinician/dental technician teamwork is of the utmost importance in achieving a successful outcome.
To summarise, existing dentures can play an important part in the following:
- Diagnosis
- Treatment planning
- Preparation of the mouth
- Impression procedures
- Recording the jaw relationship
- Denture copying
Diagnosis
A thorough assessment of a patient’s denture history and of the dentures themselves will provide key information which leads to a sound diagnosis and an effective treatment plan. Patients requesting replacement dentures fall into three broad categories.
Those wearing immediate dentures
Patients requesting replacement of their immediate dentures usually do so because the post-extraction resorption of bone has led to a loss of retention and stability. Apart from a desire for better fitting dentures, many of these patients are anxious that the appearance of the original dentures should be maintained. The clinician needs to satisfy these demands if a successful outcome is to be achieved. Improving the fit is seldom a major problem, but considerable care is needed to maintain the other well-accepted characteristics, such as position and arrangement of the artificial teeth. This challenge may best be met by using a copying technique, as described later in this chapter.
Those whose most recent dentures have been worn successfully for a significant period of time
It is important when providing new dentures for those patients whose previous dentures have been satisfactory for a number of years that the features considered to have contributed to that success are incorporated into the new prostheses. Failure to conform to this principle, which is particularly relevant to the treatment of older patients, who may adapt to change very slowly or be unable to adapt, is likely to lead to the construction of dentures which are poorly tolerated. Such failures account for a proportion of patients in the third group, who have experienced persistent denture problems.
Those with dentures that have caused persistent problems from the very beginning
For those patients with chronic denture problems, it is again vitally important to establish an accurate diagnosis. This is best achieved by asking the patient to bring in all sets of dentures in their possession so that the previous attempts can be analysed.
Within each of the three groups described, clinical situations may occur in which the clinician observes a shortcoming in the denture design which has not troubled the patient. There is then the dilemma – should the shortcoming be corrected or not? This can be a very difficult question to answer and possible pitfalls are discussed more fully under ‘Category (f)’ on p. 103. It is impossible to be dogmatic about this, particularly when treating older patients. In all instances, the clinician should consider whether it is likely to be possible to make successful new dentures if the error is retained. If it is decided to make an alteration, then it is essential to explain the reasons for this to the patient.
Treatment plan
Having assessed the patient’s dentures and related problems, the treatment plan is likely to fall into one of the following categories:
- Make temporary modifications to the existing dentures to test a diagnosis.
- Make permanent modifications to the existing dentures (e.g. rebase or modify the occlusion).
- Construct replacement dentures using conventional techniques.
- Construct replacement dentures using a copy technique for one or both dentures.
- No treatment, or referral for specialist advice. Such a decision may be made when the clinician assesses that new dentures will not overcome the patient’s complaint or where a diagnosis cannot be established with confidence, and thus there is a real risk of new dentures being no more successful than any of the existing ones.
Preparation of the mouth
Before commencing any of the treatment plans listed above, it is often necessary to carry out preparatory treatment to improve the condition of the mouth so that it is in the optimum state to receive the new prostheses. The existing dentures are often of value in carrying out this preparatory treatment – for example, when treating inflammation of the denture-bearing mucosa or when modifying an unsatisfactory jaw relationship.
Treatment of inflammation of the denture-bearing mucosa
The commonest causes of this condition are trauma from an existing denture and the proliferation of microorganisms on the impression surface of the denture. Denture trauma may be the result of an ill-fitting denture, an unbalanced occlusion, or lack of freeway space.
It is important that the inflammation of the mucosa is resolved before final impressions for the new dentures are taken. If not, the better fitting and more hygienic new dentures are likely to affect some improvement in the condition. Then, as the inflammation resolves, the shape of the denture-bearing mucosa will change causing the fit of the new dentures to deteriorate, re-establishing one of the causative factors of the original inflammation. Although the simplest method of treatment is to ask the patient not to wear the old dentures, such advice is unacceptable to the majority of patients. In such cases the dentures need to be corrected before the definitive treatment is started.
The fit of a denture can be improved quickly and effectively by temporarily relining with a short-term soft lining material (p. 234).
Occlusal imbalance can be corrected either by adjusting the occlusal surface through selective grinding or by applying a layer of cold-curing acrylic to the posterior teeth, provided this addition leaves an adequate freeway space.
Methods of eliminating infection by microorganisms are described on p. 117.
Figure 8.1 The patient is occluding on his complete dentures. Lack of maintenance has led to gross loss in occlusal vertical dimension and protrusion of the mandible.
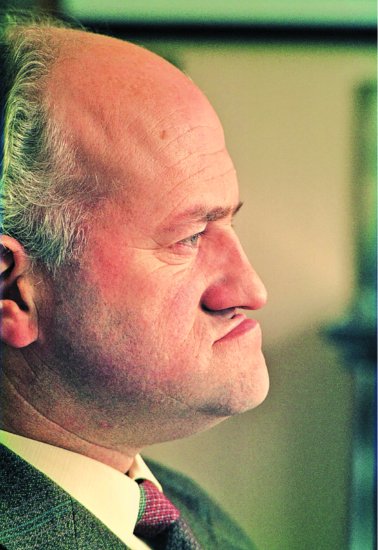
Modification of an unsatisfactory jaw relationship
Some patients still believe that once complete dentures have been provided there is no need for further treatment. This is borne out by a national survey of adult dental health in the UK which included information on the age of dentures being worn by edentulous people (Walker & Cooper 2000). A total of 39% were wearing a denture provided at least 20 years ago. Added to this was the fact that although 41% of complete denture wearers had some problem, only 13% were planning to visit a dentist. As a result, cases are seen where, through lack of maintenance, there have been considerable changes in occlusal vertical dimension and in the intercuspal position. Severe wear of the acrylic occlusal surface and resorption of alveolar bone leads to a situation where the freeway space may be 10 mm or more. Patients seeking new dentures at this advanced stage of occlusal derangement may make such statements as ‘I can’t chew my food so well’, or ‘My teeth don’t show as much as they used to’. Little imagination is required on the part of the clinician to appreciate the basis of their complaints (Fig. 8.1). However, patients are not usually aware of the problems produced in allowing the occlusion to deteriorate to such a degree.
There are two major uncertainties concerning the jaw relationship when providing replacement dentures:
1. What increase in occlusal vertical dimension is likely to be tolerated? If one attempts to reduce the freeway space to 3 mm in situations like those described above, the occlusal vertical dimension has to be increased by 7 mm or more. This may exceed a patient’s ability to adapt. For example, such a magnitude of change can result in increased masticatory stress being transmitted to the denture-bearing mucosa which might have atrophied to the extent that it is no longer able to accept such stress. Furthermore, a patient possessing a generous freeway space has been able to eat large mouthfuls of food without having to open the mandible much beyond the rest position. If the same dietary habits continue once the new dentures are fitted, difficulties in eating are likely and the increased opening of the jaw to accommodate the large mouthfuls may well produce pain in the muscles of mastication.
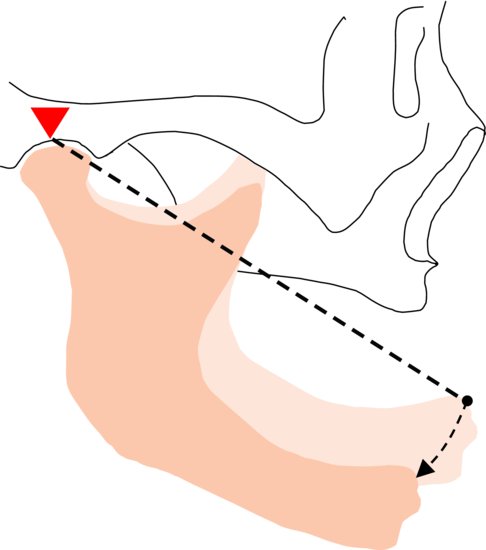
2. What is the correct jaw relationship in the horizontal plane? The reduction in occlusal vertical dimension and the unbalanced occlusion result in protrusion of the mandible. This mandibular protrusion is partly anatomical and partly habitual and generally makes it difficult, sometimes impossible, to record the retruded position. A reduction in the apparent protrusion of the mandible is, to some degree, automatic on restoration of the occlusal vertical dimension, because the hinge-like nature of the temporomandibular joint causes the chin to move posteriorly as the occlusal vertical dimension is increased (Fig. 8.2). Correcting the habitual element is usually a more gradual process. If the protrusive habit is not corrected before constructing the new dentures the subsequent gradual reduction in the protrusive posture will result in a long programme of occlusal adjustment to these new dentures.
Figure 8.2 Movement of the chin posteriorly as the occlusal vertical dimension is increased.
The uncertainties may be minimised by modifying the old dentures. The occlusal vertical dimension is increased by adding a layer of cold-curing acrylic resin to the occlusal surface of one of the dentures (Fig. 8.3). The new occlusal pattern initiates the breakdown of the habitual protrusion of the mandible as well as allowing an assessment of the patient’s ability to accept the chosen increase in occlusal vertical dimension and the change in appearance. The temporary occlusal surface can be modified to accommodate the gradual change in the jaw relationship. New dentures can then be constructed when it becomes apparent that the planned increase in vertical dimension is acceptable and the protrusion of the mandible has been corrected.
Figure 8.3 Occlusal vertical dimension corrected by the addition of a layer of cold-curing acrylic resin applied to the occlusal surface of the lower denture.
Impression procedures
Under certain circumstances an existing lower denture may be used as an impression tray to obtain the following types of master impression:
- Functional impression
- ‘Wash’ impression
- Copy of the existing impression surface of the old denture
Functional impression
A functional impression is one that is obtained by placing in the denture an impression material that exhibits plastic flow over a period of several hours. During this period the denture is worn and subjected to functional loads, e.g. during mastication. As a result the impression material records the shape of the denture-bearing tissues during function. This contrasts with the conventional impression techniques described in Chapter 10, which are in effect ‘snapshots’ of the shape of the denture-bearing tissues obtained at a single point in time. Such impressions are produced under conditions of loading applied by the clinician as the tray is seated which bear little, if any, relationship to those occurring in normal function.
An additional advantage of the functional impression technique is that it allows an assessment of the patient’s reaction to a new impression surface before proceeding with definitive treatment. For example, a patient may present with a history of persistent discomfort beneath a denture that has not responded to previous adjustments. If, after a careful evaluation of the situation, the clinician concludes that the problem is due to errors in the impression surface, it can be helpful to the clinician and reassuring to the patient to be able to test the hypothesis before being committed to definitive treatment. In the case described this can be achieved by correcting the fit of the denture with a short-term soft lining material. If the patient comments favourably on the result at the next visit, the operator has gained valuable evidence that the new impression surface is compatible with the comfortable, normal function and that a rebase or a replacement denture made to this new surface is likely to be equally well tolerated. If the patient does not comment favourably on the result the clinician can look for other possible causes of the complaint and, if necessary, remove the ineffective functional impression material. Using this approach, one is following the dictates of the saying, ‘The proof of the pudding is in the eating’. It is very important, however, to sound a note of caution here. There are situations in which a patient has persistent problems with a number of dentures in which it may be very unwise to alter the existing dentures in any way. This is discussed further in the section ‘Category (f)’ on p. 103. The short-term soft lining materials used for functional impressions are discussed more fully in Chapter 16.
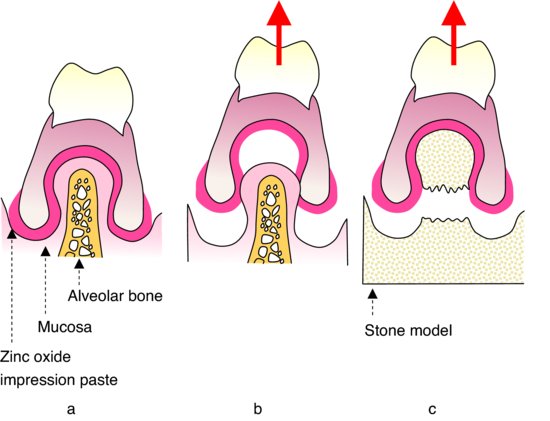
Figure 8.4 (a) Undercuts not removed from the impression surface. (b) Mucosal compressibility allows removal of the denture from the mouth. (c) Subsequent removal from the cast is impossible without damage.
The ‘wash’ impression technique
In some instances an old denture can act as a very satisfactory special impression tray. This avoids the need for a separate appointment to take a preliminary impression in a stock tray in order to construct a special tray. However, it must be appreciated that corrections of any over- or under-extension of the old denture will be required before taking the master impression. If it is necessary to increase the extension of the border by more than 2 mm, it is advisable to use one of the rigid border-trimming materials which are discussed on p. 145.
It will be appreciated that if there are significant undercuts in the impression surface of the denture they have to be removed before taking the impression for the reason described in Fig. 8.4. In most cases it is unwise to tamper with such a denture in this way for fear of making it too loose or uncomfortable to wear. Fortunately, most of the dentures for which the technique might be considered appropriate will have been originally constructed on well-resorbed ridges where undercuts do not exist.
The impression surface of the denture should be dried thoroughly to ensure that the impression material adheres firmly to the denture. Either a low viscosity silicone impression material or a zinc oxide-eugenol impression paste may be used to record the detail of the denture-bearing mucosa. Both materials are accurate when used in thin section but the former has the advantages of being tasteless, elastic and relatively clean to use. The denture is returned to the patient after the cast has been poured and the impression material has been removed.
Copying the existing impression surface of the lower denture
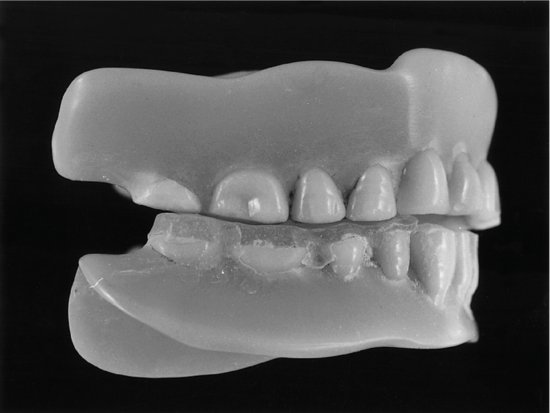
There are occasions when a new lower denture has been provided to replace an old ill-fitting one and the patient returns to the surgery with the comment that ‘the old denture was much more comfortable’.
The impression surface of the old denture may only contact the mucosa along its borders (Fig. 8.5). However, the reactions of the patient and the appearance of the mucosa show that this state of affairs is perfectly acceptable. Why do the reactions of the patient differ from the evidence of the clinical examination? It is because the denture-bearing tissues have gradually adapted to the progressive loss of fit of the old denture and the uneven distribution of load that is the result. It is also likely that the progressive loss of fit has been adequately compensated by the muscular control of the denture.
Figure 8.5 The impression surface of a lower denture which still provides comfort and />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


