Results of Periodontal Treatment
Prevention and Treatment of Gingivitis
For many years, the belief that good oral hygiene is necessary for the successful prevention and treatment of gingivitis has been widespread among periodontists. In addition, worldwide epidemiologic studies have confirmed a close relationship between the incidence of gingivitis and lack of oral hygiene.8,9
Löe and coworkers20,38 provided conclusive evidence on the association between oral hygiene and gingivitis. After 9 to 21 days without performing oral hygiene measures, healthy dental students with previously excellent oral hygiene and healthy gingiva developed heavy accumulations of plaque and generalized mild gingivitis. When oral hygiene techniques were reinstituted, the plaque in most areas disappeared in 1 or 2 days, and gingival inflammation in these areas disappeared approximately 1 week after the plaque was removed. Thus gingivitis is reversible and can be resolved by daily, effective plaque removal.
A number of long-term studies have shown that gingival health can be maintained by a combination of effective oral hygiene maintenance and scaling procedures.*
A 3-year study was conducted on 1248 General Telephone workers in California to determine whether progression of gingival inflammation is reduced in an oral environment in which high levels of hygiene are maintained.36,37 Experimental and control groups were computer matched based on periodontal and oral hygiene status, past caries experience, age, and gender. During the study period, several procedures were instituted to ensure that the oral hygiene status of the experimental group was maintained at a high level. Subjects were given a series of frequent oral prophylaxis treatments combined with oral hygiene instruction. Subjects in the control group received no attention from the study team except for annual examinations. They were advised to continue their usual daily practices and accustomed visits for professional care. After 3 years, the increase in plaque and debris in the control group was four times as great as that in the experimental group. Similarly, gingivitis scores were much higher in control subjects than in the matching experimental group. Therefore chronic marginal gingivitis can be controlled with good oral hygiene and dental prophylaxis.
Prevention and Treatment of Loss of Attachment
Prevention of Loss of Attachment
Löe et al19,20 conducted a longitudinal investigation to study the natural development and progression of periodontal disease. The first study group, established in Oslo, Norway, in 1969, consisted of 565 healthy male nondental students and academicians between 17 and 40 years of age. Oslo was selected mainly because this city had an ongoing preschool, school, and postschool dental program offering systematic preventive, restorative, endodontic, orthodontic, and surgical therapy on an annual recall basis for all children and adolescents, complete with a documented attendance record, for the previous 40 years. Members of the study population had experienced maximum exposure to conventional dental care throughout their lives. A second study group, established in Sri Lanka in 1970, consisted of 480 male tea laborers between 15 and 40 years of age. They were healthy and well built by local standards, and their nutritional condition was clinically fair. The workers had never been exposed to any programs relative to the prevention or treatment of dental diseases. Toothbrushing was unknown, and dental caries was virtually nonexistent.
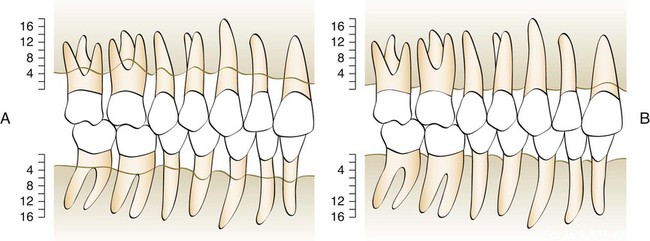
The results of this study are interesting. As the members of the Norwegian group approached 40 years of age, the mean individual loss of attachment was slightly above 1.5 mm and the mean annual rate of attachment loss was 0.08 mm for interproximal surfaces and 0.10 mm for buccal surfaces. As the Sri Lankans approached 40 years of age, the mean individual loss of attachment was 4.50 mm, and the mean annual rate of progression of the lesion was 0.30 mm for interproximal surfaces and 0.20 mm for buccal surfaces. Figure 70-1 shows a graphic interpretation of the difference between the two groups. This study suggests that without interference, periodontal lesions progress continually and at a relatively even pace.
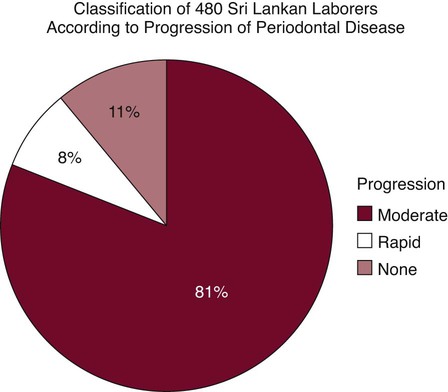
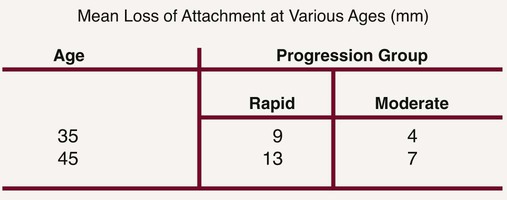
Further analysis of the Sri Lankan laborers showed that they were not all losing attachment at the same rate (Figures 70-2 and 70-3).20 Virtually all gingival areas showed inflammation, but attachment loss varied tremendously. Based on interproximal loss of attachment and tooth mortality, three subpopulations were identified as individuals with “rapid progression” (RP) of periodontal disease (8%), individuals with “moderate progression” (MP) (81%), and individuals who exhibited “no progression” (NP) of periodontal disease beyond gingivitis (11%). At age 35, the mean loss of attachment in the RP group was 9 mm; in the MP group, 4 mm; and in the NP group, less than 1 mm. At the age of 45, the mean loss of attachment in the RP group was 13 mm and in the MP group, 7 mm. Therefore, under natural conditions and in the absence of therapy, 89% of the Sri Lankan laborers had severe periodontitis that progressed at much greater rates than in the Norwegian group.
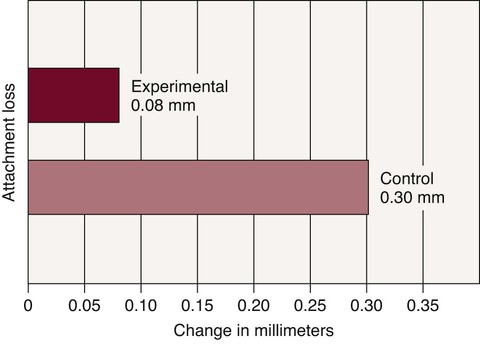
In the previously discussed study of General Telephone workers in California, loss of attachment was measured clinically and alveolar bone loss measured radiographically.36,37 After 3 years, the control group showed loss of attachment at a rate more than three times that of the matching experimental group during the same period (Figure 70-4). In addition, subjects who received frequent oral prophylaxis and were instructed in good oral hygiene practices showed less bone loss radiographically after 3 years than did control subjects. It is clear that loss of attachment can be reduced by good oral hygiene and frequent dental prophylaxis.
Treatment of Loss of Attachment
A longitudinal study of patients with moderate-to-advanced periodontal disease conducted at the University of Michigan showed that the progression of periodontal disease can be stopped for 3 years postoperatively regardless of the modality of treatment.29–32 With long-term observations, the average loss of attachment was only 0.3 mm over 7 years.30 These results indicated a more favorable prognosis for treatment of advanced periodontal lesions than previously assumed.
Another study was conducted in 75 patients with advanced periodontal disease to determine the effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health.16 This study showed that no further alveolar bone loss occurred during the 5-year observation period. The meticulous plaque control practiced by the patients in this study was considered a major factor in the excellent results produced. After 14 years, results for 61 of the initial 75 individuals were reported.14 Repeated examinations demonstrated that treatment of advanced forms of periodontal disease resulted in clinically healthy periodontal conditions and that this state of health was maintained in most patients and sites during the 14-year period. A more detailed analysis of the data, however, revealed that a small number of sites in a few patients lost a substantial amount of attachment. Approximately 43 surfaces in 15 different patients were exposed to recurrent periodontal disease of significant magnitude. The frequency of sites that lost more than 2 mm of attachment during the 14 years of maintenance was 0.8% to 0.1% per year.
Neither of these studies used a control group because failing to treat advanced periodontal patients cannot be justified for ethical reasons. However, in a study in private practice, an effort was made to find and evaluate patients with diagnosed moderate-to-advanced periodontitis who had not followed through with recommended periodontal therapy.3 Thirty patients ranging in age from 25 to 71 years were evaluated after periods ranging from 18 to 115 months. All of these untreated patients had progressive increases in pocket depth and radiographic evidence of progressive bone resorption.
In a study of the progression of periodontal disease in the absence of therapy, two different populations were monitored.18 One group of 64 Swedish adults with mild-to-moderate periodontal disease and one group of 36 American adults with advanced destructive disease were monitored but not treated for 6 years and 1 year, respectively. During the course of 6 years, 11.6% of all sites in the Swedish population (1.9% per year) showed attachment loss of greater than 2 mm, and the corresponding figure for the American population was 3.2% per year. Thus the frequency of sites with disease progression was 20 to 30 times higher in untreated groups of patients than in the treated and well-maintained groups described in the preceding discussion.18 Thus treatment is effective in reducing loss of attachment.
Tooth Mortality
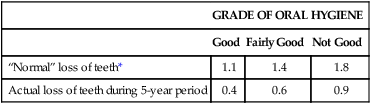
The combined effect of subgingival scaling every 3 to 6 months and controlled oral hygiene was evaluated over a 5-year period in 1428 factory workers in Oslo.22 Tooth loss was significantly reduced in all patients. This study showed that frequent subgingival scaling reduces tooth loss even when oral hygiene is “not good” (Table 70-1).
TABLE 70-1
Average Loss of Teeth during a 5-Year Period Compared with Normal Loss of Teeth in 1428 Men and Women Ages 20 through 59
| GRADE OF ORAL HYGIENE | |||
| Good | Fairly Good | Not Good | |
| “Normal” loss of teeth* | 1.1 | 1.4 | 1.8 |
| Actual loss of teeth during 5-year period | 0.4 | 0.6 | 0.9 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


