Furcation
Involvement and Treatment
The progress of inflammatory periodontal disease, if unabated, ultimately results in attachment loss sufficient enough to affect the bifurcation or trifurcation of multirooted teeth. The furcation is an area of complex anatomic morphology5,6,11 that may be difficult or impossible to debride by routine periodontal instrumentation.29,36 Routine home care methods may not keep the furcation area free of plaque17,23 (see Video 62-1: Bone Loss with Furcation).
Etiologic Factors
The primary etiologic factor in the development of furcation defects is bacterial plaque and the inflammatory consequences that result from its long-term presence. The extent of attachment loss required to produce a furcation defect is variable and related to local anatomic factors (e.g., root trunk length, root morphology)12,27 and local developmental anomalies (e.g., cervical enamel projections).22,27 Local factors may affect the rate of plaque deposition or complicate the performance of oral hygiene procedures, thereby contributing to the development of periodontitis and attachment loss. Studies indicate that prevalence and severity of furcation involvement increase with age.21,22,36 Dental caries and pulpal death may also affect a tooth with furcation involvement or even the area of the furcation. All of these factors should be considered during the diagnosis, treatment planning, and therapy of the patient with furcation defects.
Diagnosis and Classification of Furcation Defects
A thorough clinical examination is the key to diagnosis and treatment planning. Careful probing is required to determine the presence and extent of furcation involvement, the position of the attachment relative to the furca, and the extent and configuration of the furcation defect.38 The Nabors probe may be helpful to enter and measure difficult to access furcal areas (Figure 62-1). Transgingival sounding may further define the anatomy of the furcation defect.29 The goal of this examination is to identify and classify the extent of furcation involvement and to identify factors that may have contributed to the development of the furcation defect or that could affect treatment outcome. These factors include (a) the morphology of the affected tooth, (b) the position of the tooth relative to adjacent teeth, (c) the local anatomy of the alveolar bone, (d) the configuration of any bony defects, and (e) the presence and extent of other dental diseases (e.g., caries, pulpal necrosis).
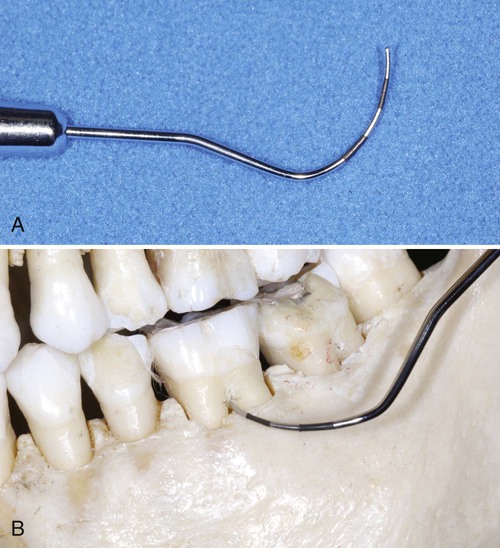
The dimension of the furcation entrance is variable but usually quite small; 81% of furcations have an orifice of l mm or less, and 58% are 0.75 mm or less.5,6 The clinician should consider these dimensions, and the local anatomy of the furcation area,11–13 when selecting instruments for probing. A probe of small cross-sectional dimension is required if the clinician is to detect early furcation involvement.
Local Anatomic Factors
Clinical examination of the patient should allow the therapist to identify not only furcation defects but also many of the local anatomic factors that may affect the result of therapy (prognosis). Well-made dental radiographs, although not allowing a definitive classification of furcation involvement, provide additional information vital for treatment planning (Figure 62-2). Important local factors include anatomic features of the affected teeth, as described next.

A, Grade I furcation on the mandibular first molar and a grade III furcation on the mandibular second molar. The root approximation on the second molar may be sufficient to impede accurate probing of this defect. B, Multiple furcation defects on a maxillary first molar. Grade I buccal furcation involvement and grade II mesiopalatal and distopalatal furcations are present. Deep developmental grooves on the maxillary second molar simulate furcation involvement in this molar with fused roots. C, Grades III and IV furcations on mandibular molars.
Root Trunk Length
A key factor in both the development and the treatment of furcation involvement is the root trunk length. The distance from the cementoenamel junction to the entrance of the furcation can vary extensively. Teeth may have very short root trunks, moderate root trunk length, or roots that may be fused to a point near the apex (Figure 62-3). The combination of root trunk length with the number and configuration of the roots affects the ease and success of therapy. The shorter the root trunk, the less attachment needs to be lost before the furcation is involved. Once the furcation is exposed, teeth with short root trunks may be more accessible to maintenance procedures, and the short root trunks may facilitate some surgical procedures. Alternatively, teeth with unusually long root trunks or fused roots may not be appropriate candidates for treatment once the furcation has been affected.
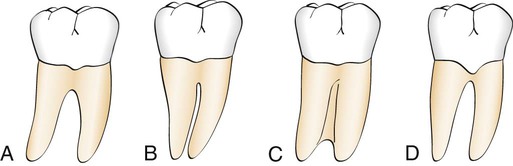
A, Widely separated roots. B, Roots are separated but close. C, Fused roots separated only in their apical portion. D, Presence of enamel projection that may be conducive to early furcation involvement.
Root Length
Root length is directly related to the quantity of attachment supporting the tooth. Teeth with long root trunks and short roots may have lost a majority of their support by the time that the furcation becomes affected.13,20 Teeth with long roots and short-to-moderate root trunk length are more readily treated because sufficient attachment remains to meet functional demands.
Root Form
The mesial root of most mandibular first and second molars and the mesiofacial root of the maxillary first molar are typically curved to the distal side in the apical third. In addition, the distal aspect of this root is usually heavily fluted. The curvature and fluting may increase the potential for root perforation during endodontic therapy or complicate post placement during restoration.1,25 These anatomic features may also result in an increased incidence of vertical root fracture. The size of the mesial radicular pulp may result in removal of most of this portion of the tooth during preparation.
Anatomy of Furcation
The anatomy of the furcation is complex. The presence of bifurcational ridges, a concavity in the dome,11 and possible accessory canals16 complicates not only scaling, root planing, and surgical therapy,28 but also periodontal maintenance. Odontoplasty to reduce or eliminate these ridges may be required during surgical therapy for an optimal result.
Cervical Enamel Projections
Cervical enamel projections (CEPs) are reported to occur on 8.6% to 28.6% of molars.26,27,35 The prevalence is highest for mandibular and maxillary second molars. The extent of CEPs was classified by Masters and Hoskins27 in 1964 (Box 62-1). Figure 62-4 provides an example of a grade III CEP. These projections can affect plaque removal, can complicate scaling and root planing, and may be a local factor in the development of gingivitis and periodontitis. CEPs should be removed to facilitate maintenance.

Anatomy of the Bony Lesions
Pattern of Attachment Loss
Other Dental Findings
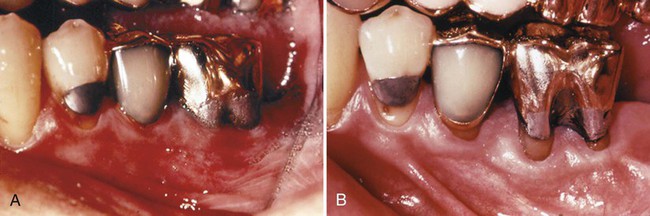
The dental and periodontal condition of the adjacent teeth must be considered during treatment planning for furcation involvement. The combination of furcation involvement and root approximation with an adjacent tooth represents the same problem that exists in furcations without adequate root separation. Such a finding may dictate the removal of the most severely affected tooth or the removal of a root or roots (Figure 62-5).
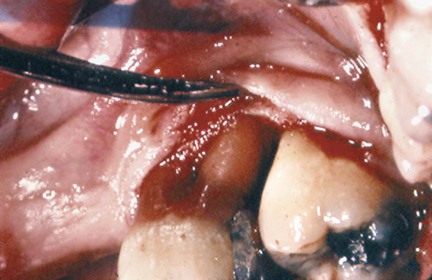
Note the buccal furcation, which communicates with the distal furcation of a maxillary first molar that also displays advanced attachment loss on the distal root and approximation with the mesial root of the maxillary second molar. The patient with such teeth may benefit from root resection of the distobuccal root of the first molar or extraction of the molar.
Indices of Furcation Involvement
The extent and configuration of the furcation defect are factors in both diagnosis and treatment planning. This has led to the development of a number of indices to record furcation involvement. These indices are based on the horizontal measurement of attachment loss in the furcation,14,17 on a combination of horizontal and vertical measurements,37 or a combination of these findings with the localized configuration of the bony deformity.10 Glickman14 classified furcation involvement into four grades (Figure 62-6).
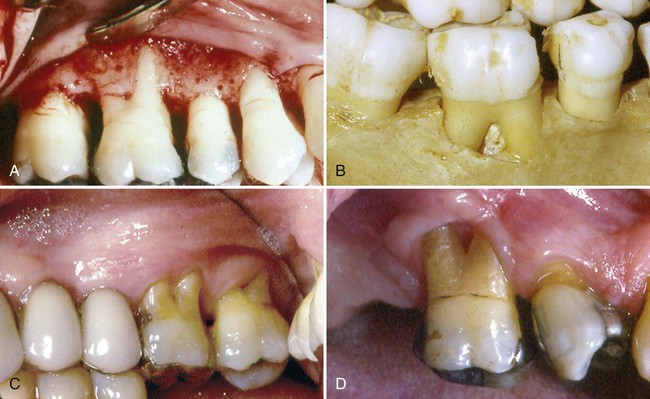
A, Grade I furcation involvement. Although a space is visible at the entrance to the furcation, no horizontal component of the furcation is evident on probing. B, Grade II furcation in a dried skull. Note both the horizontal and the vertical component of this cul-de-sac. C, Grade III furcations on maxillary molars. Probing confirms that the buccal furcation connects with the distal furcation of both these molars, yet the furcation is filled with soft tissue. D, Grade IV furcation. The soft tissues have receded sufficiently to allow direct vision into the furcation of this maxillary molar.
A, This mandibular first molar has been treated endodontically and an area of caries in the furcation repaired. A Class II furcation is present. B, Results of flap debridement, osteoplasty, and severe odontoplasty 5 years postoperatively. Note the adaptation of the gingiva into the furcation area. (Courtesy Dr. Ronald Rott, Sacramento, CA.)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


