4
The oral presentation of toothwear in adults
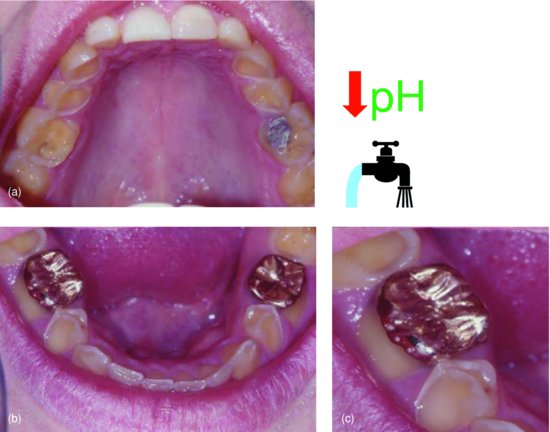
Toothwear processes are active at different times in the life of an individual and differ from person to person. As considered in the preceding chapters, some patients may have a large amount of tooth structure loss occurring early in life, whilst others do so at a later stage. In either case, all patients with toothwear have alternating stages of stability and progression throughout their lifespan. The presentation of toothwear in adults is thus a cumulative result of all the events leading to the state of the dentition at the time of presentation. The case shown in Fig. 4.1 highlights how progression of toothwear processes challenges even the most technically sound restorations, when patient compliance is lacking, their lifestyles continue to challenge their dentition and when the underlying aetiology may not have been fully appreciated during the assessment and diagnostic stages.
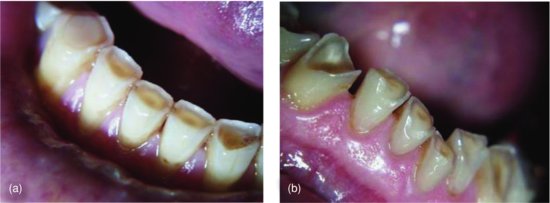
Figure 4.1 Severe toothwear in a 22-year-old male patient affecting tooth surfaces across the dentition. The patient reported a partygoing lifestyle, regular binge drinking, frequent vomiting and high volumes of acidic beverage consumption over the past 5 years. He admitted drinking no water throughout the day and instead resorted to acidic beverages. He was aware of a severely dry mouth particularly at rave parties when resorting to recreational drugs. Severe erosion affected the palatal surfaces of the maxillary teeth (a). Gold onlays were placed on the mandibular first molar teeth (b) at the age of 17 years as his dentist suspected a bruxism habit and had a splint made, which he has worn every night since fabrication. Since placement, severe erosion processes have undermined the gold onlays, (c) and the adjacent premolar has lost extensive tooth structure. (From Young, 2003a, with permission of Erosion Watch Pty Ltd.)
DIAGNOSTIC MODALITIES
For correct prevention, management and possibly restorative intervention, if required, to be implemented, correct identification of toothwear lesions, toothwear processes and underlying aetiology is paramount. Diagnostic and assessment modalities used to identify dental caries are inappropriate and differ substantially from those applied to toothwear (Table 4.1).
Diagnostically, no one tool exists to detect dental erosion or toothwear, making visual identification and evaluation of clinical appearance essential (Lussi et al. 2009). Those diagnostic modalities useful in the detection of dental caries have limited application in the assessment of toothwear and are more applicable to general patient examination to exclude other dental anomalies. Radiographs are of benefit to identify or exclude the presence of interproximal caries or assess the state of periodontal bone support across the dentition. Transillumination and laser diagnostic modalities are of assistance in the diagnosis of dental caries. The worn dentition however requires a different approach based on assessment of the hard and soft tissues, examination of the dentition and charting of toothwear (Table 4.2). The examination of extraoral and soft tissue features detailed in Chapter 1 is paramount, often providing valuable insight and diagnostic information in elucidating the multifactorial aetiology underlying toothwear processes in an individual. Hence, even prior to examination of the dentition, the astute clinician may identify extraoral or soft tissue signs relevant to the diagnostic assessment process. A good clinical history will further assist in identifying contributing dietary, health and lifestyle factors. Whilst clinical photographs provide some aesthetic reference points, study models provide an important and appropriate baseline reference point that may be compared to at subsequent recall appointments over time or when new study models are taken every 2 years.
Table 4.1 Diagnostic modalities for toothwear and dental caries.
| Diagnostics | Toothwear | Dental caries |
| Tactile probing | Of little significance | May further damage porous enamel or fissures and only limited sources still recommend probing |
| Transillumination, laser diagnostics | Of little application | Useful for detecting decay in interproximal, pit and fissure regions |
| Radiographs | Of little significance other than excluding other pathologies | Important to check for interproximal lesions and ascertain depth of decay |
| Presence of plaque and tartar | Is encouraging as it is suggestive of salivary remineralisation potential | Important to identify presence at surfaces at risk of decay |
| Saliva tests: Flow rate, buffering capacity, pH, bacterial counts |
Toothwear patients often in good health but suffer sports- or work-related dehydration. Confirms medically induced xerostomia. | Beneficial to ascertain at-risk status |
| Study models | Important for most cases to assess worn surfaces and consider vertical dimension | Of little benefit unless rampant decay requires complex rehabilitation |
| Clinical photography | Appropriate in all cases with significant aesthetic bearing | Appropriate in all cases with significant aesthetic bearing |
| Existing restorations | High margins provide a record of dental erosion since placement | Record of past caries experience Check marginal leakage |
| Clinical history | Very important | Less important |
| Pulp testing | Rarely required | Frequently indicated |
Table 4.2 Examination of toothwear and dental caries.
| Diagnostics | Toothwear | Dental caries |
| Extraoral examination | Facial features: eyes, ears Complexion of skin, lips, hair Parotid regions, TMJ |
Of little significance except subcutaneous abscesses or sinuses |
| Intraoral soft tissue examination | Sialadenosis Linea alba Salivary glands Tongue indentations |
Of little significance Dento-alveolar abscesses |
| Intraoral hard tissue examination | Visual inspection of: Incisal/occlusal, buccal/palatal surfaces for wear Charting of toothwear |
Visual inspection for white-spot lesions, staining and cavitation DMFS or DMFT charting of dentition |
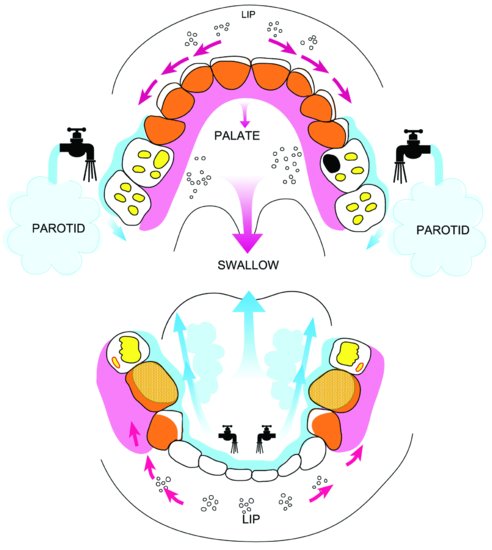
Figure 4.2 Conceptualisation of toothwear across the dentition of the 22-year-old male patient depicted in Fig. 4.1. States of repeated dehydration, use of recreational drugs, frequent vomiting and high acidic beverage consumption combined to result in severe dental erosion in this patient. Whilst lingual surfaces of the mandibular teeth have been protected, the minimal saliva available afforded little protection against the highly acidic and repeated insults on the dentition for the maxillary anterior palatal and mandibular posterior buccal surfaces, which have been severely affected by dental erosion. (From Young, 2003a, with permission of Erosion Watch Pty Ltd.)
SURFACE SUSCEPTIBILITY OF TOOTHWEAR AND SITE SPECIFICITY OF DENTAL CARIES
Lesions of toothwear affect the dentition in a surface-specific manner (Khan et al. 1998, 1999, 2001). Lesions occur in certain areas more than others, not so by chance, but for reasons of variations in exposure levels of different surfaces to extrinsic and intrinsic acids, elements of abrasion, attrition and salivary protection (Young & Khan 2002). Appreciating how these elements affect certain parts of the dentition more so than others helps in understanding how the worn dentition a patient presents with has developed and what processes may be involved. Identifying toothwear on particular teeth across the dentition and more specifically on different tooth surfaces assists in conceptualising thought processes to elucidate the underlying aetiologies (Fig. 4.2).
Tooth surfaces are differently affected by toothwear and dental caries. Interproximal regions are almost never affected by attrition and erosion, yet are susceptible to develop dental caries. Whilst considerable wear on approximal surfaces has been documented in aboriginal dentitions (Kaidonis et al. 1992), toothwear in modern-day societies is different from that experienced in historic civilisations (Young 1998). Modern dietary trends do not promote such excessive wear on approximal surfaces, and in the majority of cases, they can be considered negligible. On maxillary anterior teeth, wear facets develop on incisal edges, marginal ridges and cingula as the palatal surfaces are also occluding surfaces (Fig. 4.3). As severity of erosion and attrition increases further, tooth structure on the palatal surfaces is lost. Maxillary anterior teeth are often found devoid of enamel surface palatally in patients with high exposure to dietary or intrinsic acids. Dental caries, however, does not affect the occluding surfaces and instead may form in any deep palatal pits or fissures. It is rare to see decay on wear facets, even if dentine is exposed, as plaque has limited opportunity to evolve and develop on occluding surfaces. Mandibular anterior teeth may develop wear facets chipped and worn regions of dental erosion incisally, but are rarely affected by caries on these surfaces. Further, given the salivary protection offered by the submandibular glands, toothwear on lingual surfaces of the mandibular anterior teeth is rare.
In molar teeth, the regions of the occlusal surfaces affected by attrition and erosion also vary from those affected by dental caries (Fig. 4.4). Attrition affects the cuspal inclines and tips. Erosion results in cup- or bowl-shaped lesions on the cuspal apices and inclines. Caries affects fissures on the occlusal surface and buccal pits. Similar to anterior incisal surfaces, attrition facets are sites that are not prone to dental caries, and interproximal regions susceptible to dental caries are rarely affected by toothwear. Such surface- and site-specific differences further highlight the different processes resulting in the various types of tooth structure loss. Toothwear and dental caries are clearly different processes. The patterns by which tooth structure is lost vary by segment of teeth and site across the dentition and even on individual surfaces (see Figs. 4.3 & 4.4). This surface specificity has restorative and dental material selection implications discussed in later chapters and also requires different approaches to the charting of such lesions. Application of caries assessment techniques to areas of toothwear to characterise the different lesions of non-carious tooth surface loss is inappropriate.
Figure 4.3 The incisal edges and palatal surfaces affected by attrition (a) or erosion (b) are contrasted with sites susceptible to caries (c) on an upper first permanent incisor. Wear facets on the incisal edge, marginal ridges and cingulum characterise attrition. The incisal edge and marginal ridges are hollowed out in cases of erosion. Palatal pits are sites susceptible to dental caries. (From Young & Khan, 2009, with permission from Erosion Watch Pty Ltd.)
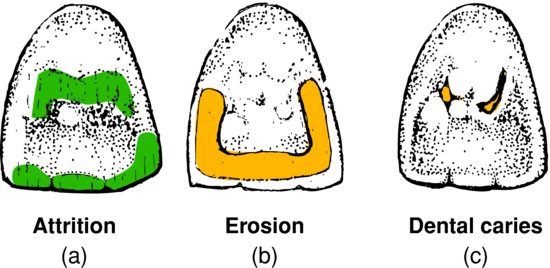
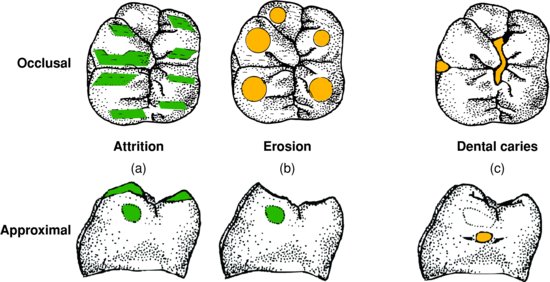
Figure 4.4 The five cusps of a lower first permanent molar, surfaces affected by attrition (a) or erosion (b), are contrasted with sites of pit and fissure caries (c). Wear facets on the cusp slopes and marginal ridges characterise attrition. Cusp apices develop bowl-shaped lesions through processes of erosion. Buccal pits and occlusal fissures are sites prone to the development of dental caries. (From Young & Khan, 2009, with permission from Erosion Watch Pty Ltd.)
THE CLINICAL PRESENTATION OF TOOTHWEAR
Having introduced the differences in surface specificity, consideration is next given to the clinical presentation of toothwear across the dentition. Clinically, given the limited diagnostic modalities available, in the assessment of toothwear heavy emphasis is placed on visual identification. A strategy for identifying toothwear is detailed based on morphology of toothwear lesions of different surfaces. Scanning electron microscopy techniques have offered valuable insight into the descriptive parameters required to characterise lesions, describe subtle changes on the tooth surface and form the basis from which the identification strategy presented has been developed over the past decade. High-magnification microscopy techniques allow detailed visualisation of ultrastructural components, whilst lower magnification microscopy techniques provide type specimens for occlusal and incisal attrition and erosion, cervical lesions, and areas of lesion fusion, involving both occlusal and cervical surfaces.
Attrition
Facets of attrition by definition are flat, well defined and demarcated (Fig. 4.5). They appear shiny to visual inspection, especially following recent active progression. Matching facets are often identified in opposing teeth, as wear progresses from tooth-to-tooth interaction. Whilst identification may be easier on a set of study models, when examining a patient’s dentition directly, it is important to dry the tooth surface fully to allow better visualisation. Matching facets can also be identified by asking the patient to lightly occlude on a piece of articulating paper. Facets on the palatal slopes of maxillary anterior teeth often extend in an incisal-to-apical direction due to the upward and backward movement of the lower incisor teeth in normal occlusion. Whilst wear of the mamelons of newly erupted incisor teeth in children is physiologic, multiple wear facets across the dentition are the first sign of a patient being at risk of developing significant toothwear. Well-marked mesial and/or distal facets on the incisal edges of canine teeth reflect the more anterior indentation of the lower on the upper canine. In premolar and molar teeth, the mesial and distal slopes of the cusps and the marginal ridges are the common surfaces where facets usually develop. The mesiobuccal cusp of the upper first permanent molar teeth develops a facet over the central fissure between the mesio- and distobuccal cusps of its lower counterpart in normal occlusion (Angle class I malocclusion). Attrition involves the earliest forms of tooth structure loss and often simultaneously the least amount volumetrically. Teeth in contact undergo physiologic wear throughout their lifetime. Areas of heavy contact wear gradually. The physiologic balance across the dentition is hence maintained over a lifetime and is not a static process.
Figure 4.5 Mild attrition on the incisal edges of maxillary anterior teeth (a). Lower anterior teeth with moderate attrition on the incisal edges (b) exposing dentine. Facets are shiny, flat, highly polished and well demarcated (c).

In areas of attrition, as shown in Fig. 4.6, dentine is exposed in accordance with the Greaves effect (1973). The leading-edge enamel protects the adjacent dentine and a shallow slope is formed. Dentine is scooped out in front of the trailing-edge enamel. This describes the Greaves effect, which has been used to deduce the direction of the chewing stroke on fossil teeth (Greaves 1973). These shallow differences in contour can be seen on the incisal edge wear facet of the incisor illustrated in Fig. 4.6a. The literature will continue to debate the limited role of bruxism in some cases of toothwear and the sometimes-severe attrition that may result and a detailed consideration of the literature on the topic is presented in Chapter 10.
Figure 4.6 Scanning electron micrograph of a maxillary left second incisor with incisal attrition (a). The shallow leading edge (LE) enamel-to-dentine interface contrasts with the hollowed and chipped dentine-to-enamel interface of the trailing edge (TE). The arrow on the incisal edge indicates the orientations of striae. The cingulum (C) shows compression pits consistent with wear in centric occlusion. When an opposing tooth produces a wear facet that penetrates to dentine, the direction of travel of the opposing tooth can be deduced from the contours on the dentine within the facet (b), as leading-edge enamel (LE) protects the adjacent dentine and a shallow slope is formed. Dentine is scooped out in front of the trailing-edge enamel (TE). This is termed ‘Greaves effect’ (Greaves 1973). (From Young & Khan, 2009, with permission from Erosion Watch Pty Ltd.)
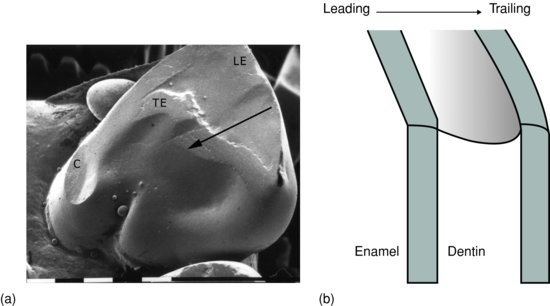
Figure 4.7 Mandibular anterior teeth with moderate dental erosion. Cupping or scooping of dentine on the incisal edges is notable, and the lower right canine has been restored previously with high restorative margins and further loss of surrounding tooth structure since placement of the restoration is evident (a). Sharp enamel peripheries and chipping are common as erosion progresses (b).
Erosion
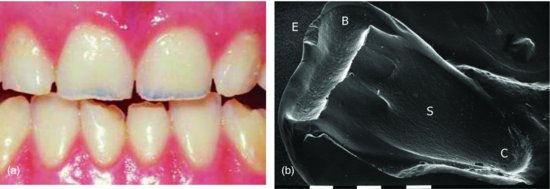
The appearance of dental erosion differs markedly from attrition. On the incisal edges of the incisor teeth, thin enamel margins and peripheries are prone to chipping (Fig. 4.7). The dentine is deeply scooped out and lesions are not as well defined. On maxillary incisor teeth, in addition to thinning of the incisal edge, the palatal surface is susceptible to erosion (Fig. 4.8).
Figure 4.8 Dental erosion on the incisal edges of maxillary incisor teeth is visible from the facial perspective as bluish-grey regions of translucency through the thinned enamel shell remaining (a). (From Young & Messer, 2002, with permission of Dentil Pty Ltd.) Scanning electron micrograph of a maxillary left lateral incisor with erosion of the incisal edge (B) and palatal surface (C) extending to the gingival margin (b). The facial enamel is chipped (E) due to softening and lack of support from the hollowed-out incisal dentine (B). Striations (S) on the palatal surface indicate attrition and abrasion of softened dentine. The cingulum is lost and erosion extends into the gingival crevice (C) (Bar = 1 mm). (From Khan et al., 1998, with permission from the Australian Dental Journal.)
Dental erosion on the molar and premolar teeth characteristically involves cup- or bowl-shaped lesions. Cup-shaped lesions are symmetrical dentine exposures affecting the cuspal apices and inclines (Fig. 4.9). Margins of existing restorations may stand proud of surrounding tooth structure. Progression of occlusal dental erosion results in merger of cup-shaped lesions across the oblique and marginal ridges to ultimately affect the entire occlusal surface and form a bowl-shaped lesion (see Fig. 1.8b). Unlike facets, cuspal-cupped lesions do not match where the upper and lower teeth meet in occlusion. The mandibular molar teeth are far more severely affected compared to the opposing maxillary molar teeth and are an important indicator of early-onset dental erosion in children (Khan et al. 2001).
Microscopy helps explain why cup-shaped lesions are symmetrical. Figure 4.10a shows rods of enamel run in bands parallel to one another. One band, the parazone, cuts across another zone, the diazone. Parazones and diazones are alternating Hunter–Schreger bands within enamel (Osborn 1990). This complex arrangement of enamel rods gives the cusp tip its high-impact strength to resist the high forces of chewing and prevents it cracking under stress over the tip of the crown dentine (D). As shown in Fig. 4.10b, these alternating bands spiral down from the very tip of the cusp. When the spirals are cut in longitudinal section, their complexity results in the gnarled appearance to the enamel on the tip. Whilst the cusp tips are highly resistant to masticatory forces, when sustained acids etch the gnarled enamel, the symmetry of the spirals is revealed and the dentine becomes exposed, forming cup-shaped lesions.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


