1
The multifactorial nature of toothwear
TOOTHWEAR PROCESSES
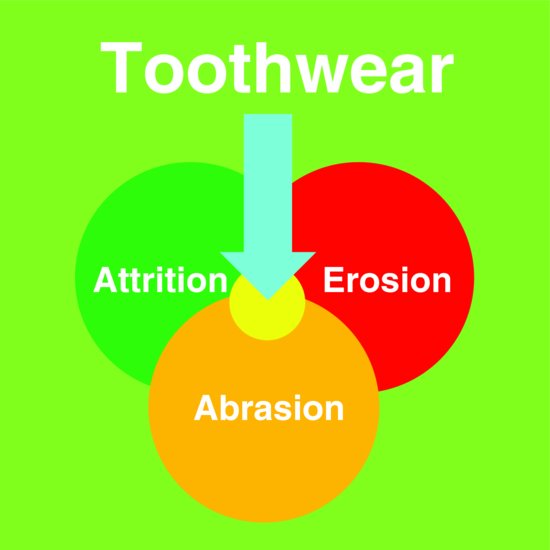
Attrition, erosion and abrasion describe wear processes (Fig. 1.1). Attrition involves two-surface (tooth-to-tooth) wear. Erosion, less commonly referred to as corrosion, results from acidic dissolution of mineralised tooth structure. Abrasion on a surface comprises wear from externally applied particles or objects.
When a patient presents with a heavily worn dentition (Fig. 1.2), the clinician considers whether the toothwear processes have involved elements of attrition, erosion or abrasion. Whilst the wear facets identified on the lower anterior teeth suggest attrition, numerous high margins on restorations point to involvement of erosion, removing tooth structure adjacent to these restorations. Demineralisation of tooth structure further predisposes to abrasion as evident in cervical regions, many of which have previously been restored. Since placement of these restorations, toothwear processes have continued. This case highlights that interrelationships exist between toothwear processes which potentiate one another.
Although the processes of attrition, erosion and abrasion can be simulated under laboratory conditions, clinically these processes do not occur independently (Fig. 1.3). The coarse particles of foods in primitive diets potentiated the wear facets (Young 1998) of attrition by abrasion (Fig. 1.3a). Modern diets lack such abrasives; however, oral acids that cause erosion demineralise enamel and dentine, potentiating attrition and abrasion (Figs. 1.3b & c). A recent literature review on erosion noted that dietary acids are considered by many researchers probably to be the most common cause of acid erosion (Bartlett 2009). Exaggerated wear facets are the first sign of erosion-potentiated attrition in young adults’ permanent teeth. Toothbrush and toothpaste combinations are important considerations, particularly in patients in whom dental erosion has also been identified, for abrasiveness becomes potentiated when tooth structure is demineralised. A combination of these two processes can lead to severe toothwear (Fig. 1.4). When used on demineralised tooth structure, abrasion from routine use of standard toothbrushes and toothpaste formulations is significant, whilst in the absence of erosion, it is considered to be minimal (Addy 2005). Attritional facets and cuspal-cupped lesions can be found on the same tooth (Fig. 1.5). This suggests that the wear facet worn by the mesiobuccal cusp of the upper first molar has been potentiated or exaggerated by occlusal erosion that has produced the cuspal-cupped lesions. Moreover, erosion has produced the shallow cervical lesion on the buccal surface of this tooth possibly potentiated by toothbrush abrasion.
Figure 1.1 The processes of attrition, erosion and abrasion: (a) Attrition is wear between two tooth surfaces. (b) Erosion is tooth surface loss from acids. (c) Abrasion is loss of tooth surface from a foreign body.
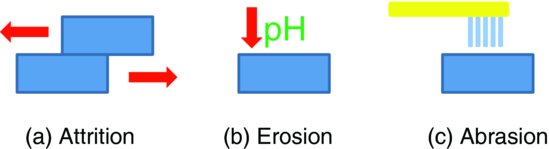
Figure 1.2 Three processes of toothwear are reported in this case: (a) Incisal attrition on incisors. (b) Occlusal erosion on premolars and molars and around amalgam restorations. (c) Various cervical regions have been restored previously, with further loss of tooth structure since the time of restoration. (From Young, 2001, with permission of Dentil Pty Ltd.)

Figure 1.3 Interactions of abrasion, attrition and erosion in toothwear: (a) Acids soften surfaces potentiating attrition. (b) Acids soften surfaces potentiating abrasion. (c) Abrasion from particles harder than enamel and dentine potentiates attritional wear.
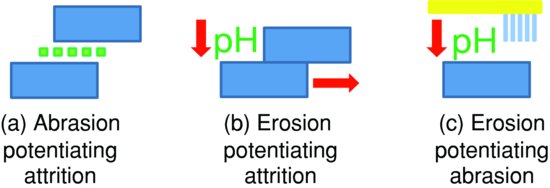
Figure 1.4 Facial surfaces of the central incisors are devoid of enamel in a 31-year-old female gymnast. The dentine is deeply grooved by toothbrush abrasion. The approximal enamel is remarkably intact. Scanning electron microscopy (SEM) (Bar = 1 mm). (From Khan et al., 1999, with permission from the Australian Dental Journal.)
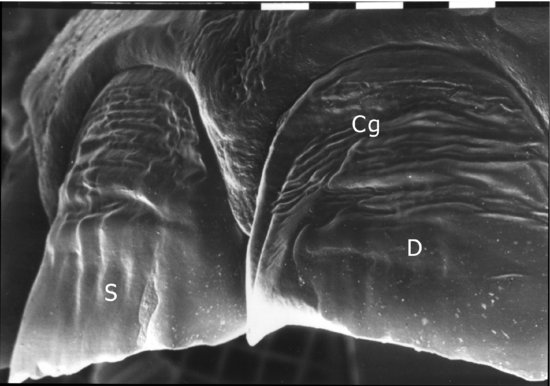
Figure 1.5 An attritional wear facet (F) on a buccal cusp of a lower first permanent molar. On all cusps are the cupped lesions of erosion not necessarily associated with attrition. A shallow buccal cervical lesion (C1) is also present on this tooth (Bar = 1 mm). (From Young & Khan, 2009, with permission from Erosion Watch Pty Ltd.)
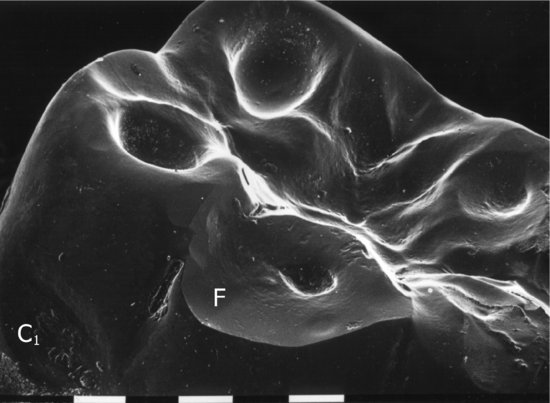
Figure 1.6 Toothwear is best conceptualised as a combination of erosion, attrition and abrasion.
These interrelationships between attrition, erosion and abrasion highlight that multifactorial processes create a worn dentition (Fig. 1.6). Each patient has a variation in the involvement of attrition, erosion and abrasion. In many patients, it is predominantly underlying erosion that potentiates the secondary effects of attrition and abrasion. Appreciating that different processes are working concurrently allows the clinician to focus diagnostic, preventive and management strategies on all three aetiologies. Thus, tooth tissue loss will continue if its multifactorial nature is not recognised and addressed.
SALIVA PROTECTION
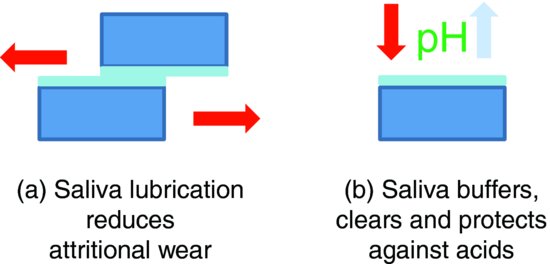
Saliva is central in counteracting and balancing toothwear processes, and tooth surfaces are protected against toothwear by salivary buffering capacity, salivary pellicle, acid clearance and washing of the dentition (Dawes 2008). The unstimulated flow rate of saliva and salivary buffering capacity have been directly associated with dental erosion (Zero & Lussi 2005). Both mucous and serous saliva protect against attritional wear through lubrication of the teeth and areas of interarch contact, as well as neutralise acids within the oral environment. Saliva also reduces demineralisation by its content of calcium and phosphate (Fig. 1.7).
Figure 1.7 Saliva offers protection against attritional wear (a) through lubrication and (b) by raising the pH through buffering and clearance of acids that produce erosion.
INTRINSIC AND EXTRINSIC ACIDS
Acids that demineralise teeth are extrinsic dietary or intrinsic, gastric or plaque in origin. Dietary acids most commonly implicated are ascorbic acid (vitamin C), citric acid, sodium citrate and orthophosphoric acid, because these are used as flavours and preservatives in most acidic beverages. So, soft (Johansson et al. 2002), sports (Milosevic 1997) and energy drinks are sources, with other acids in wines. Hydrochloric acid from gastric juice is the usual intrinsic acid implicated in dental erosion and toothwear (Scheutzel 1996). A study examining 19 professional wine tasters found mild-to-severe dental erosion and found the subjects with severe dental erosion also to have had a history of gastritis or reduced salivary flow rate and/or buffering capacity (Wiktorsson et al. 1997).
Figure 1.8 A 24-year-old male patient with a long history of athletic training at a professional level. Acidic beverage rehydration frequently occurred subsequent to intense physical training sessions, at times of dehydration and low salivary protection. This allowed rapid loss of tooth structure to occur. (a) Near exposures of the pulpal tissues are evident on the lingual surfaces of the maxillary anterior teeth. (b) Extensive areas of erosion have notably affected his first molar teeth. (c) Cervical lesions are evident on the maxillary and mandibular buccal surfaces of canine and lateral incisor teeth. (From Young, 2003b, with permission of Dentil Pty Ltd.)

The case presented in Fig. 1.8 shows the toothwear of an elite athlete, 24 years of age. His lifestyle placed him at risk of developing severe toothwear. His rigorous training regimes reduced the salivary protection of his dentition. Subsequent rehydration with acidic sports drinks at times of dehydration affected his dentition. Acidic beverages and foods are important contributors to erosive toothwear in many individuals (see Chapter 3), given their common availability, and yet the pH alone is insufficient to determine their erosive potential, which is instead influenced by a large range of variables including consumption patterns, adhesion and chelating properties of salivary protection, and swallowing and clearance patterns (Lussi et al. 2004). Frequent episodes of reduced saliva protection and acid drinks resulted in severe loss of enamel and dentine in this young adult, principally from dental erosion. Dental erosion in athletes is a growing concern (Sirimaharaj et al. 2002); however, many children and young adults also frequently consume such beverages. Increased consumption of sports drinks and acidic beverages, during the day and also during heavy exercise, is likely contributing to the increasing dental erosion prevalence (ten Cate & Imfeld 1996), particularly in young individuals.
EXAMINATION OF FACIAL, EXTRAORAL AND INTRAORAL SOFT TISSUES
The multifactorial nature of toothwear is further highlighted by benefits from identifying facial, extraoral and intraoral soft tissue features even before a worn dentition is assessed. Much can be learned of lifestyles, general medical conditions, temporomandibular joint (TMJ) disorders and salivary gland pathology by considering signs and symptoms relevant to toothwear. For the clinician, a schematic approach for examination of facial, extraoral and intraoral features adds diagnostic information relevant to the aetiology of the patient’s condition. Icons applicable to these features are included to trigger the clinician’s mind during the examination (Fig. 1.9). These icons are used throughout this text alongside clinical photographs of interesting cases to indicate additional findings. Visual inspection and manual palpation are all the clinical skills the clinician needs to make additional important observations. The icons remind us to record the relevant ones. The odontogram (Fig. 1.9, centre) describes each tooth as an icon. Three surfaces of each tooth are represented, as approximal surfaces are almost never significantly affected by toothwear and consequently the clinician need only record the severity of wear on the occlusal and cervical surfaces illustrated. Detailed methods for examination of the worn dentition are provided in Chapter 4.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


