10
The role of toothwear in occlusion
This chapter discusses various aspects of occlusion in relation to toothwear based on an evaluation of the available literature. As background information, some relevant historical perspectives on the subject are provided.
Extensive toothwear seems to have been the norm in ancient societies, with factors such as dietary habits, food composition and its preparation, and age being among its main contributory factors (Johansson et al. 2008). The consequences went beyond extensive deterioration of occlusal morphology to include notable changes in dentoalveolar and craniofacial morphology over a lifetime. These changes are considered to have maintained an efficient masticatory system, which was vital for survival (Hylander 1977). The effects on craniofacial morphology of excessive function, quite apart from occlusal and proximal toothwear, are primarily passive tooth eruption, lingual tilting of the anterior teeth and an anterior rotation of the mandible, resulting in a more ‘edge-to-edge’ anterior relationship (Begg & Kesling 1977; Hylander 1977; Johansson 1992; Fig. 10.1).
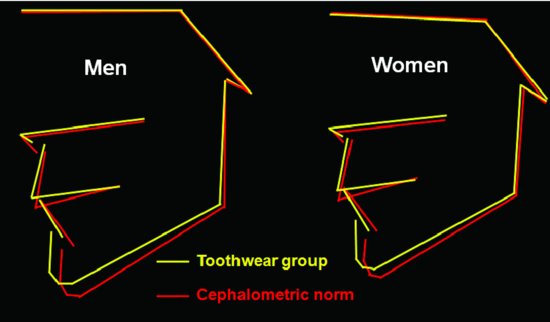
The frequency of malocclusions in primitive man is lower than in his modern counterpart, and it has been speculated that this resulted from attrition-caused alterations in the dentofacial morphology. Low frequencies of crowding, impacted molars, rotations, amongst others, in primitive populations can be attributed to the substantial gain of space in the dental arch following proximal attrition, thus preventing space-related malocclusions (Begg & Kesling 1977). As wear progresses, different opinions have been expressed as to whether facial height is reduced or whether it is unaffected. It is likely that this depends on the rate at which toothwear is occurring: if the rate is slow, compensatory dentoalveolar growth mechanisms will compensate for the decrease of facial height caused by the shortening of teeth, while if there is a rapid toothwear, these mechanisms may not be able to fully compensate and the occlusal vertical dimension (OVD) may be reduced. Begg and Kesling (1977) speculated that the facial height of modern Western man increases during life because of a lack of attrition. That facial height increase in adulthood has indeed been confirmed in several studies (Kollias & Krogstad 1999). However, whether the sole cause for this is an absence of attrition is not clear. Changes of craniofacial morphology similar to those observed in ancient materials have also been found in modern high-wear subjects (Fig. 10.2; Kiliaridis et al. 1995). The anthropological observations described provide some insight into causation, progression and features of severe toothwear. The similarities they show with today’s patients with severe toothwear are remarkable and may to an extent contextualize the outcomes seen both before and after attempts at managing such conditions in today’s patients. In addition, the continuing alteration of craniofacial morphology is also of significance to explain the infraposition sometimes seen in implant-supported crowns (Thilander 2009).
Figure 10.1 Development of an edge-to-edge bite in a contemporary 50-year-old Saudi man. (With permission from Johansson & Carlsson 2006.)

Figure 10.2 Mean facial diagrams of men and women in occlusal wear samples and cephalometric norm values. (With permission from Kiliaridis et al. 1995.)
In historical skull materials, toothwear was a more common cause of tooth damage and tooth loss than either dental caries or periodontal disease (Fig. 10.3). In Egyptian mummies, almost all abscesses in the jaws were ascribed to toothwear and only a fraction to caries. Even though toothwear in modern man is usually far less extensive, its impact on patients’ satisfaction with their dentition can be severe and affect their quality of life (Al-Omiri et al. 2006).
Figure 10.3 Extensive toothwear of maxillary teeth in a medieval man estimated to be 35–45 years old. The loss of the first right molar was most certainly caused by wear penetrating into the pulp, subsequently leading to an inflammatory process in the periapical jawbone. (By courtesy of Dr. M. Wretemark, editor of S:t Per i Skara, a book on excavations of a medieval graveyard in the Swedish town Skara, published in Swedish 2010; photograph taken by L.G. Olsson.)

In the anthropological literature, it has been assumed that toothwear had a linear progression, so that it could be used for age determination in historical skull materials (Fig. 10.4; Wedel et al. 1998).
Figure 10.4 Mandibular teeth from a medieval person with estimated age 25–35 years. Some crowding in the premolar regions and extensive toothwear on the first molars, but no caries. (With permission from Wedel et al. 1998.)

Figure 10.5 Casts of Australian aborigines showing increasing toothwear with age. (With permission from Beyron 1964.)
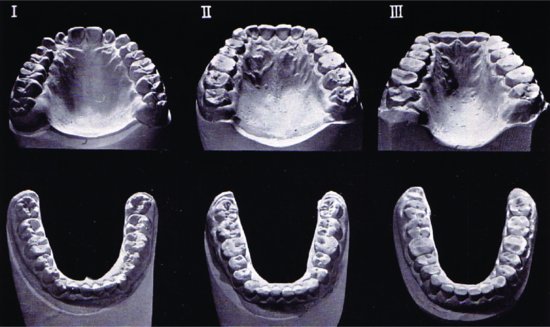
The linearity of its progression is evident also in contemporary populations before they adopted Western lifestyles, e.g. in the Australian aborigines some 50 years ago, as described by Beyron (1964; Fig. 10.5).
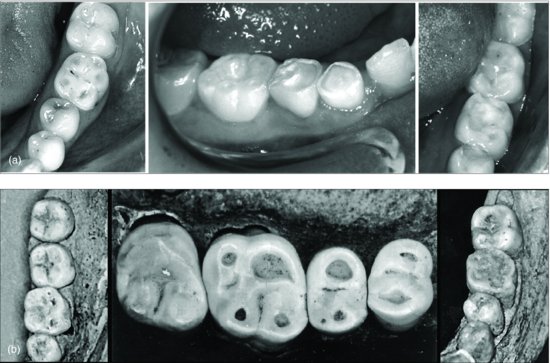
In contrast to linear progression, modern man more likely experiences ‘bursts’ of wear, coinciding with the presence of certain causative factors, which can explain part of the widely differing severities and patterns of wear found in people today, and even amongst those of the same age (Johansson 2002). Today, dental erosion is widely considered to be a major cause of toothwear (Bartlett 2005), yet the morphological features of the wear seen show a remarkable similarity with those seen in our ancestors (Figs. 10.6a & b).
DEVELOPMENT OF OCCLUSION
Comparative anatomy demonstrates wide differences among species in tooth morphology and occlusion, jaw architecture, muscles and temporomandibular joints (TMJ). The differences can be related to, and indeed reflect, variations in functional activities, and in turn, have evolved over millions of years in response to needed adaptations to type of diet and the role of feeding (Creanor & Noble 1994). In comparison, modern humans (Homo sapiens) have a relatively short history (30 000–40 000 years) but have roots that reach back much earlier. Among the differences between modern man and early hominids is the relative proportion of cranium to jaws due to both an increase in cranium size and a decrease in jaw size in H. sapiens. A change in feeding habits, in addition to, and also coupled with the ‘mechanisation’ brought about by the use of hand-held tools has been suggested to be the major factor in the reduction in tooth size as well as the modification of the lower part of the face during evolution.
Figure 10.6 Severe toothwear with ‘cuppings’ in a contemporary patient (a) and in an ancient skull (b) (18). Note how closely the patterns and distributions of wear resemble each other. (With permission from Johansson & Carlsson 2006.)
The deciduous and mixed dentitions
At the age of about 8 months, the first deciduous teeth erupt, generally beginning with the mandibular central incisors. Then follow the other maxillary and mandibular incisors, and at about 16 months of age, the deciduous first molars erupt. By the time that the first molars intercuspate, dental occlusion is established for the first time. The eruption of the deciduous dentition and occlusion are usually complete around 2.5 years of age (Ingervall 1988). There is considerable growth of the jaws and alveolar processes during the first years of life, which provides space for the erupting deciduous teeth, and in many children there is also a surplus of space resulting in small gaps between the deciduous teeth. After the eruption of all deciduous teeth, the most marked change is that of progressive toothwear that can be substantial in many children. Weak-to-moderate correlations have been shown between wear facets on anterior primary teeth at 5 years of age and those of their permanent successors at age 14 and 18 (Nyström et al. 1990). It has also been reported that subjects with erosive lesions in their primary dentition have a significantly increased risk for toothwear in the permanent dentition (Ganss et al. 2001). A follow-up study of children and adolescents over 20 years of age found that toothwear at 15 years of age predicted increased anterior toothwear at age 35 (Carlsson et al. 2003). Furthermore, clinical observations indicate that occlusal erosion and toothwear in the deciduous dentition can influence the developing dentition and adversely affect OVD and craniofacial development (Fig. 10.7; see also Chapter 1, Fig. 1.14).
Figure 10.7 Extensive toothwear (combination of attrition, probably bruxism and erosion, caused by gastroesophageal reflux) of the deciduous dentition in a 12-year-old girl, which has created unfavourable alveolar compensatory growth of the posterior segment, thus affecting the occlusal vertical dimension. (With permission from Johansson & Carlsson 2006.)
The mixed dentition starts when the permanent first molars erupt and the deciduous mandibular incisors are exfoliated, on average at 6 years of age. There is some variation in the order of eruption of the permanent teeth, but in general, the first molars and the incisors in both jaws will have erupted by 8.5 years of age. From age 10 the canines and premolars start erupting, with some differences in their sequence between the jaws. At age 12 the second molars erupt, after which there is a pause up to around age 20 when the eruption of the third molars, the wisdom teeth, usually occurs.
In young adults, the normal occlusal plane is established by the permanent incisors and the first molars. Enamel wear facets that may develop do not affect the overbite, overjet or the OVD substantially (Fig. 10.8).
Figure 10.8 In young adults, the normal occlusal plane is established by the permanent incisors and the first molars. Enamel wear facets that may develop do not affect the overbite, overjet or OVD substantially.
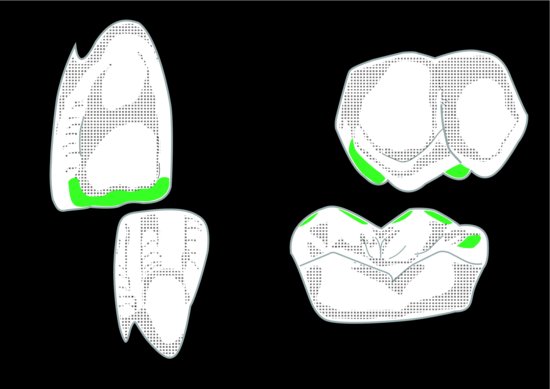
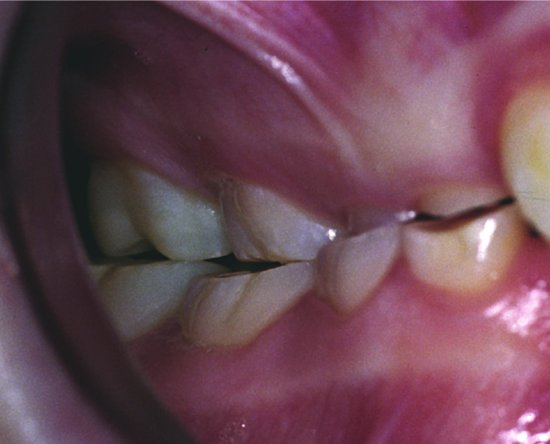
However, as stated above, there is a correlation between the severity of wear on the deciduous teeth/mixed dentition with that found on the permanent teeth later in life in untreated patients. So, it comes as no surprise that many patients in their early teens may, in addition to exaggerated wear facets on their permanent teeth, also have developed toothwear of the incisal edges and erosion on marginal ridges of the upper central incisors and cuspal-’cupped’ lesions on their lower first permanent molars. If this proceeds unchecked, the entire palatal surfaces of the incisors are degraded and the entire occlusal surfaces of the lower molars become eroded (Fig. 10.9). This may lead to a change in the OVD, needing therapeutic considerations (see below).
Figure 10.9 The palatal surface of the upper incisor is degraded. The large mesiopalatal cusp of the upper first molar and the five cusps with the entire occlusal basi/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


