Lymphatics and Spread of Dental Infection
• To discuss briefly the function of the lymphatic system
• To diagram and label the major groups of lymph nodes that drain the teeth and the oral cavity
• To define the terms primary, secondary, and tertiary nodes of involvement as they relate to lymph drainage
• To name the primary lymph drainage of all the teeth
• To discuss briefly the concept of fascial space infection
• To discuss briefly how a fascial space infection may spread from the oral cavity to the thorax
LYMPHATIC SYSTEM
Distribution Pattern
We will now examine the distribution pattern of these channels and nodes and discover how they relate to the head and neck area. Fig. 35-1 shows some of the major groups of nodes in the head and neck. The nodes are grouped together into small clusters, which are all interconnected by channels. Each group drains fluids from certain structures or tissue areas, which explains why lymph nodes are involved in combating infections in areas of the body. A sore throat, for example, can be followed by tenderness in the neck and finally a tender lump in that area. In such an instance the infection from the throat has spread through the lymph channels and nodes behind the throat wall known as retropharyngeal nodes. From there it travels through lymph vessels until reaching the first group of lymph nodes in the neck known as upper deep cervical nodes. The lymphocytes in the node have begun to combat the infection and also have started to multiply, causing the node to become enlarged and tender. If the infection is successfully combated in that node, it will subside; however, if the infection is great, it may spread through that lymph node or nodes and on to the next node or group of nodes.
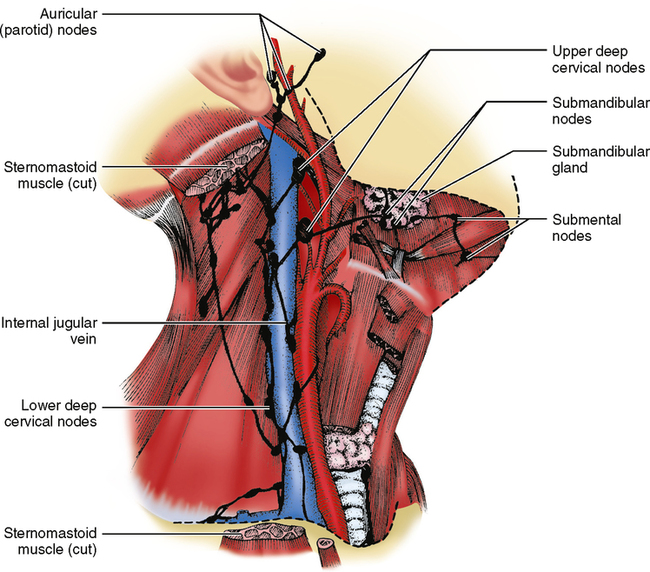
NODE GROUPS AFFECTED BY DISEASE
The terms primary nodes, secondary nodes, and tertiary nodes are often used in discussions about infections and cancer, both of which spread through lymphatic channels. These terms refer to the groups of nodes that are affected in a disease process. If an infection is not stopped by the first (primary) group of nodes, it will spread to the second (secondary) group. If it is not stopped there, it may spread to the third (tertiary) group. One node or group of nodes can be primarily involved in one source of infection, and the same group of nodes can be secondarily or tertiarily involved in another source of infection. Look at the upper deep cervical nodes (see Fig. 35-1). An infection of the third molars may involve these nodes first—the primary group involved. If the infection were in a first molar, the initial sign of infection would be in the submandibular nodes; if it were not successfully combated there, it would spread secondarily to the upper deep cervical nodes. Infections originating in the middle of the lower lip would spread first to the submental nodes, secondarily to the submandibular nodes, and then to the upper deep cervical nodes, which in this instance would be tertiary nodes of involvement. Keep in mind that in infections, any group of nodes may overcome the infection if it is not too severe, and the infection may go no farther.
SPREAD OF INFECTION IN FASCIAL SPACES
How can one predict where the infection will go? Refer to Fig. 26-17, a medial view of the body of the mandible, and picture the lengths of the roots of the individual teeth. Look at the mylohyoid line on the mandible and notice its location relative to the apices of the roots. You can see that, in general, the apices of the mandibular molar teeth are inferior to the mylohyoid line, whereas the apices of the roots of premolars and the anterior teeth are above the mylohyoid line. Therefore a molar infection will tend to break out of the bone below the mylohyoid line and spread to the space beneath the chin, referred to as the submental space. Infections of the premolars and the anterior teeth will tend to break out of bone above the mylohyoid line and spread to the spaces in the floor of the mouth, referred to as the sublingual space.
1. What is the function of lymph nodes?
2. What are the major groups of lymph nodes in the head and neck?
3. Name the structures that drain primarily into each group of lymph nodes.
5. Where may fascial space infections eventually end up if left untreated, and how serious could this be?
6. Submental space infections come from which group of teeth?
7. Swelling below the eye would come from infection in which teeth?
8. What group of nodes would first be noticed as being painful in a throat infection?
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


