CHAPTER 3
Alveolar Distraction Osteogenesis
Hasten slowly.
—Augustus Caesar
Following tooth loss, resorption of the alveolar ridge occurs in both the vertical and horizontal direc-JL tions. Most of this resorption occurs during the first 6 months after tooth removal. In the maxillary and mandibular anterior segments, rapid resorption of the buccal plate occurs. Resorption of the posterior segment occurs later.1,2 Although dental rehabilitation of partially and fully edentulous patients with dental implants is a reliable and common practice at present,3–5 unfavorable local ridge conditions may prevent dental implant placement.
In the past, complicated laboratory techniques, including the use of pink porcelain to give the impression of shorter teeth, were used in an attempt to compensate for lack of facial bone in esthetic implant sites. Today, these techniques are generally not necessary and are considered unacceptable in the esthetic zone. Rather, to correct this dual vertical and horizontal resorption, several surgical approaches have been proposed: autogenous bone grafts,6,7 guided bone regeneration,8,9 and alveolar distraction osteogenesis (ADO).10–14
Presently, the most widely used method for increasing bone volume is bone graft augmentation, using either autogenous, allogeneic, or xenogeneic bone graft material. The problem with bone augmentation, however, is its unpredictability. Resorption of bone grafts almost always occurs, and as much as 40% to 60% of the augmented bone can be completely resorbed over time. Other disadvantages of bone grafting are insufficient soft tissue coverage, donor site morbidity, and prolonged healing time before implant placement.
Alveolar crest distraction is a relatively new technique for restoring bony height of a resorbed alveolus. Over the past decade there have been enough reports of alveolar distraction to begin a critical evaluation of the various approaches to ADO, including unidirectional, bidirectional, and width distraction, to establish criteria for its use.


 Unidirectional Crest Distraction
Unidirectional Crest Distraction
Alveolar ridge distractors can be classified according to location, intraosseous or extraosseous; according to direction of distraction, unidirectional or bidirectional; and by alveolar widening or lengthening. Uckan et al33 compared intraosseous and extraosseous ADO and found no statistically significant difference in complication rate between the two methods. Therefore, the clinician is free to choose an ideal size and type of distractor according to the defect’s size and shape, the patient’s tolerance, and the distance to the opposing arch. What is most important is that the device be applied atraumatically and that the distraction osteotomy and distraction process be done as physiologically as possible.
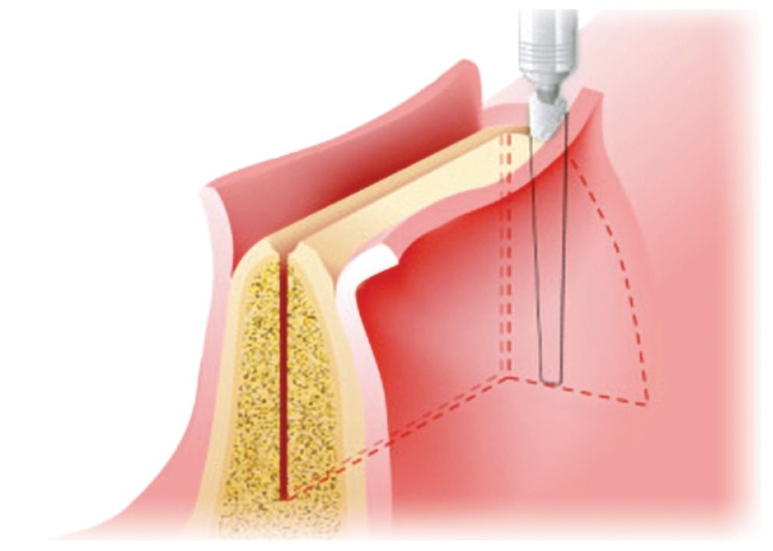
The desired result of alveolar distraction is the transportation of a segment of mature bone to lengthen the alveolus for implant anchorage, to improve esthetics, and to satisfy the functional prosthetic requirements. Preservation of the periosteum and the endosteal blood supply is critically important to the osteogenic potential of the distraction zone. Therefore, the mucosal incision must be placed in the vestibule rather than at the alveolar crest, and the periosteum must be elevated minimally. The lingual or palatal mucoperiosteum and soft tissue must be left intact and must not be detached from the transport segment. The osteotomy design of the transport segment should be slightly trapezoidal, for “draw,” but the segment also should be as large as possible so that osseous integrity is not compromised.
During distraction, there is a tendency for palatal or lingual alveolar deflection to occur because of mucoperiosteal traction during lengthening. A countertraction device can be attached to teeth or two distraction devices can be used, one at each edge of the bone segment, to help overcome vector deflection. Generally, two devices allow better control of vector.
Case 1: Severe alveolar vertical deficiency following trauma to the anterior maxilla
A 16-year-old patient was involved in a motor vehicle accident that caused dentoalveolar fractures of teeth and avulsion of several anterior maxillary teeth and associated bone. Some months later, the intraoral view revealed a severe vertical deficiency of the alveolar bone that did not permit placement of implants (Fig 3-1a).
After the initial treatment with maxillomandibular fixation, DO of the anterior maxilla was planned. An incision, designed with minimal periosteal detachment to preserve vascularity of the transport segment, was made at the depth of the sulcus. A trapezoidal segmental osteotomy was performed, and a central unidirectional distraction device was secured with miniscrews (Figs 3-1b and 3-1c).
After a 5-day latency period to allow primary callus organization, the distraction device was activated at a rate of 0.5 mm per day until the desired vertical height was achieved. During the initial distraction, a tendency for palatal shifting caused by mucoperiosteal traction was observed. Therefore, a tooth-borne suspension device was mounted to the distractor (Fig 3-1d). A vertical distraction of 12.0 mm proceeded (Fig 3-1e) and was followed by 10 weeks of retention to allow bony maturation and mineralization. The distraction device was removed, and an additional 4 weeks of healing ensued (Fig 3-1f).
Five dental implants were placed when healing was completed (Fig 3-1g). After a 6-month osseointegration period, a fixed dental prosthesis was placed (Fig 3-1h). Panoramic radiographs taken before and after distraction demonstrated the segmental bone movement as well as successful implant placement (Figs 3-1i to 3-1l).
Case 1: Severe alveolar vertical deficiency following trauma to the anterior maxilla

Fig 3-1a Patient presents for treatment several months after avulsion of maxillary anterior alveolar bone and teeth. A vertical deficiency of alveolar bone prevents the placement of implants.
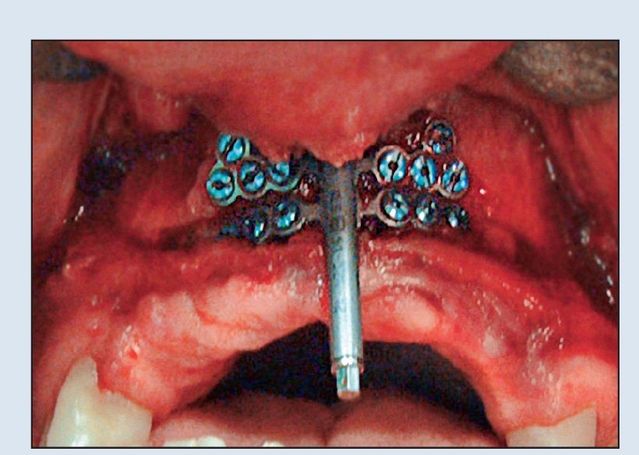
Fig 3-1b A trapezoidal segmental osteotomy is performed, and the distraction device is fastened by miniscrews.
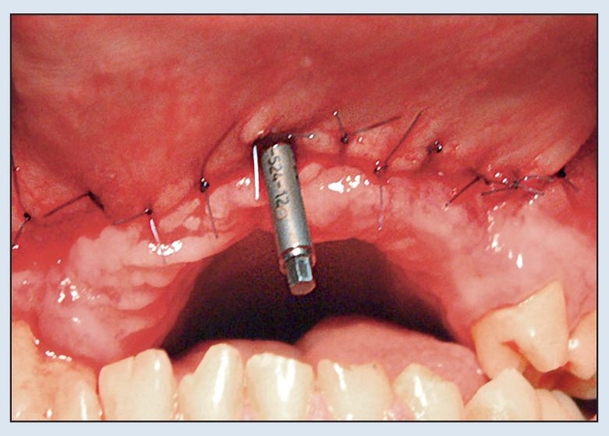
Fig 3-1c A central unidirectional crest distractor is placed.
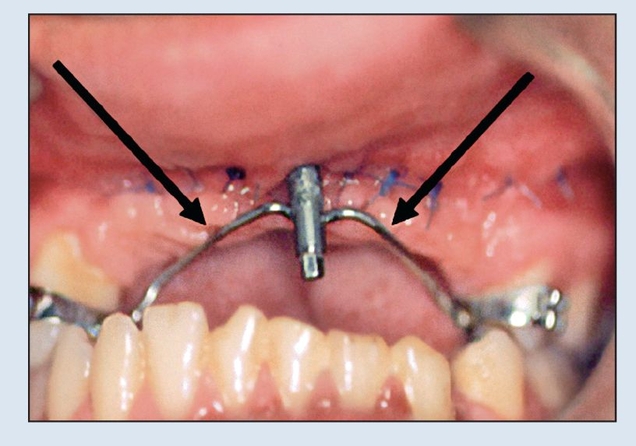
Fig 3-1d Tooth-borne counter suspension (arrows) of the distractor is used to prevent deflection to the palatal.

Fig 3-1e Vertical distraction of 12.0 mm has been accomplished.

Fig 3-1f The healed maxillary anterior segment shown 4 weeks after device removal, at the time of implant placement (5 months’ healing).
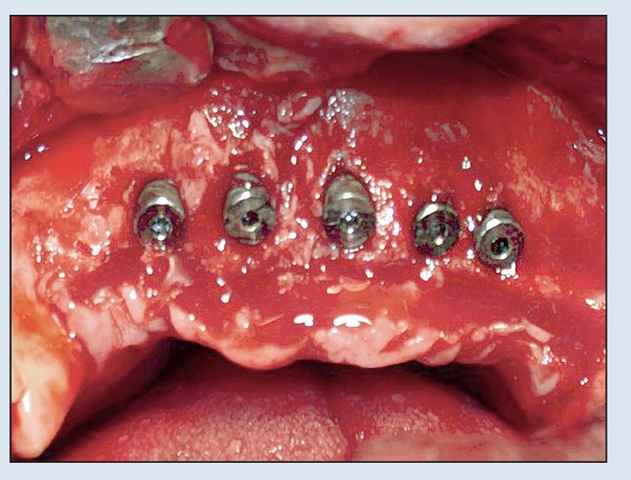
Fig 3-1g Five implants are placed after the vertical crest lengthening.

Fig 3-1h The definitive dental restoration is a functional and esthetically pleasing six-unit prosthesis.
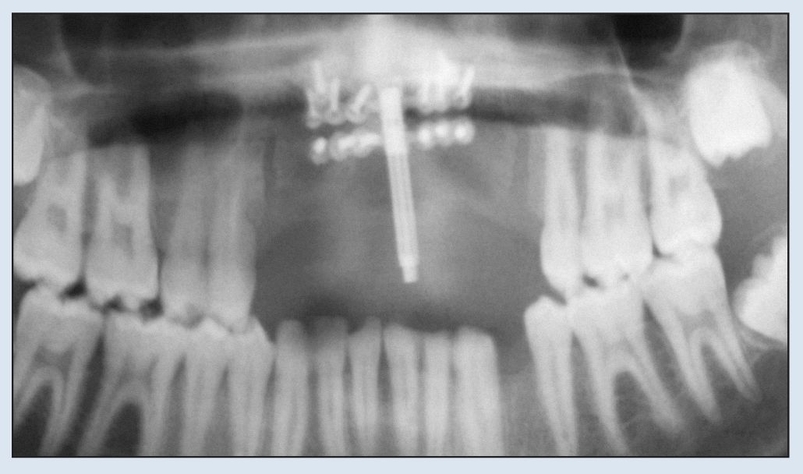
Fig 3-1i The central unidirectional alveolar distractor before vertical distraction.

Fig 3-1j The restored crest after 12.0 mm of vertical distraction.
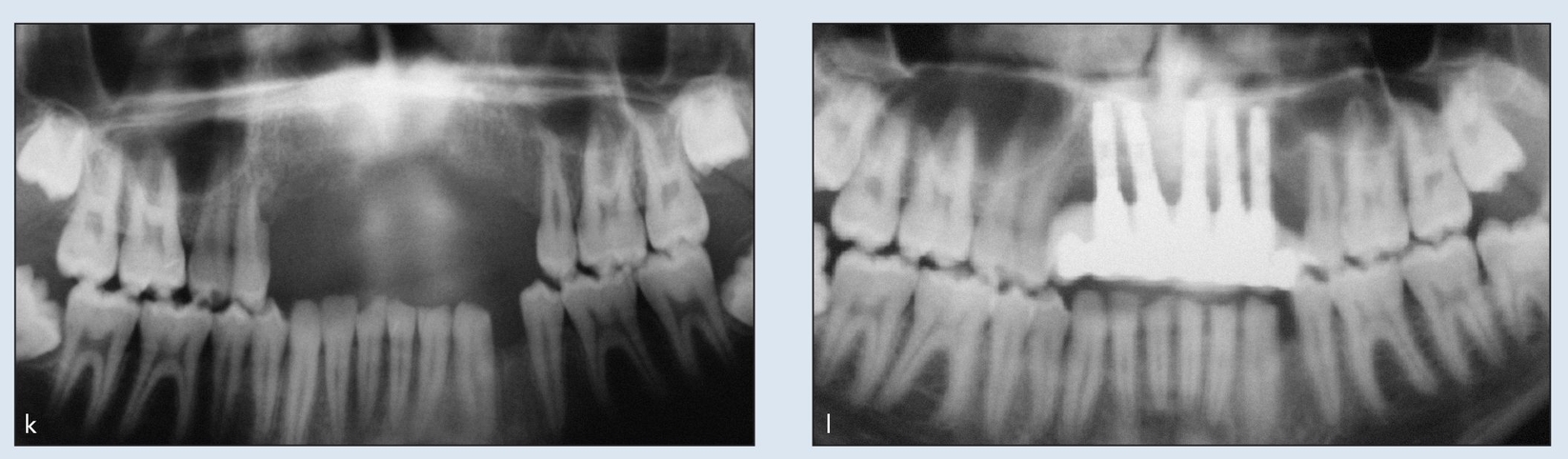
Figs 3-1k and 3-1l (k) Pretreatment vertical deficiency of the maxillary anterior alveolar bone. (l) The maxillary anterior segment restored, after 12.0-mm distraction, with implants and the definitive prosthesis.
Case 2: Vertical deficiency following avulsion of anterior maxillary teeth
A 23-year-old patient was referred after treatment for traumatic symphyseal mandibular fracture and avulsion of anterior maxillary teeth and the alveolar supporting bone. The mandible was treated with open reduction and placement of two miniplates. The examination revealed a maxillary vertical deficiency of the alveolar bone that prevented placement of implants (Fig 3-2a).
DO of the remaining anterior maxillary bone was planned. An incision was made deep in the sulcus; to pre serve the vascularity of the transport segment, bone detachment was minimized. A trapezoidal segmental osteotomy was performed. To overcome the palatal traction of the vector of lengthening, two distraction devices were placed at the edges of the distracted bone and coun-tersupported by the teeth (Figs 3-2b and 3-2c).
Case 2: Vertical deficiency following avulsion of anterior maxillary teeth

Fig 3-2a Patient shown after traumatic avulsion of maxillary anterior teeth and the alveolar supporting bone. Maxillary vertical deficiency of the alveolar bone prevents the placement of implants.
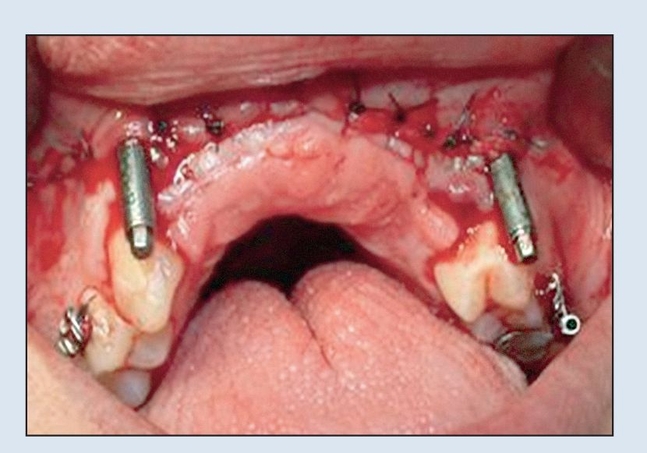
Fig 3-2b A trapezoidal segmental osteotomy is performed, and two unidirectional distraction devices are connected.

Fig 3-2c Two devices allow better control of the vector of lengthening.

Fig 3-2d At the end of vertical lengthening of 12.0 mm, the defect is closed.

Fig 3-2e Alveolar crest shown after the removal of distraction devices.
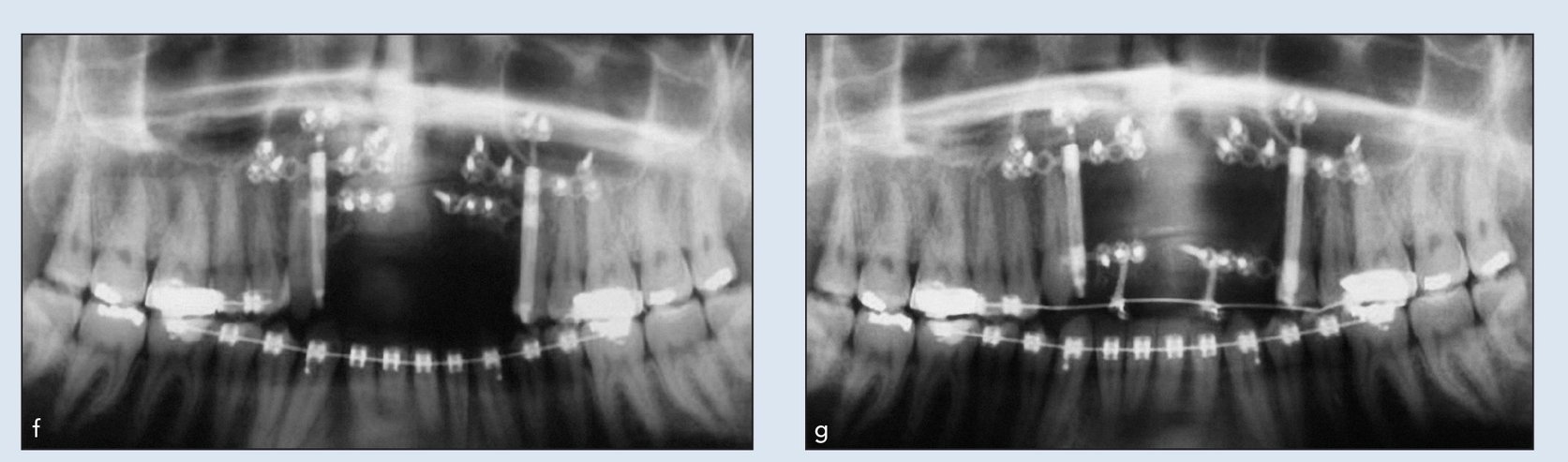
Figs 3-2f and 3-2g Panoramic radiograph of (f) the two devices before lengthening and (g) the 12.0-mm vertical lengthening.
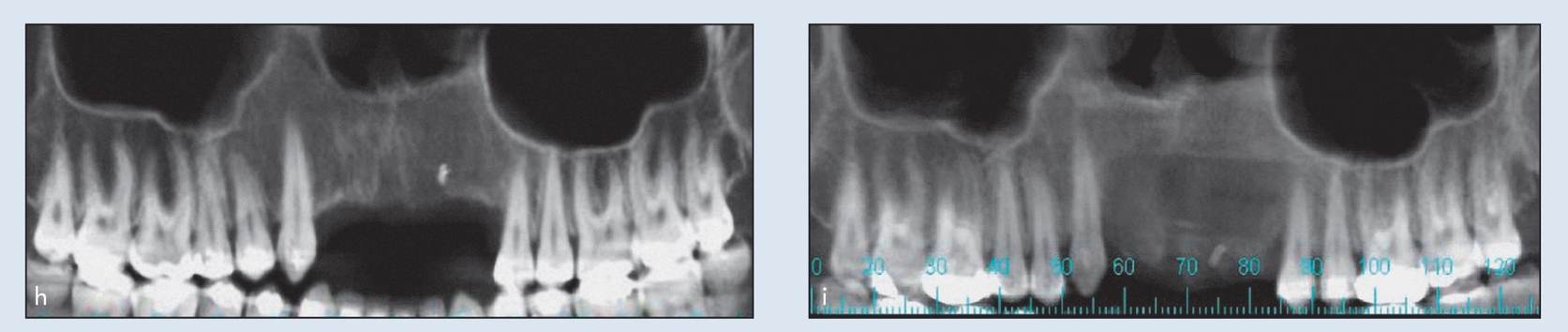
Figs 3-2h and 3-2i (h) CT showing the deficient alveolar crest before distraction. (i) CT taken 3 months after the distraction, before placement of the implants, demonstrating the newly distracted bone.
After 5 days of latency, the two distraction devices were activated once a day at a rate of 0.5 mm per day until the desired vertical alveolar height was achieved. The application of two devices allowed better control of the vector of lengthening. A vertical distraction of 12.0 mm was achieved (Fig 3-2d). After an additional 10 weeks of retention for bony maturation and mineralization, the two distraction devices were removed (Fig 3-2e).
After an additional 4 weeks of healing, four dental implants were introduced in the newly distracted bone. Panoramic radiographs and computed tomograms (CTs) taken before and after treatment revealed the segmental bone movement, the newly distracted bone, and implant placement (Figs 3-2f to 3-2i).
 Bidirectional Crest Distraction
Bidirectional Crest Distraction
With unidirectional distractors, distraction is possible in the vertical direction only. Often, unidirectional distractors require the assistance of other means, such as orthodontics, to pull the bone transport segment buccally against the traction of the periosteum. With the bidirectional crest distractor (2DCD, Surgi-Tec), however, distraction can be performed buccolingually as well as in the vertical direction. The 2DCD consists of three main parts: a baseplate; a threaded cylinder and a small screw for locking the cylinder into the baseplate; and a horizontal module with two retracting pins that connect via the vertical screw to the cylinder.
Before the distractor is placed, the ideal tooth position is determined on study casts by the use of denture teeth and pink wax. The size of the defect can also be determined by noting the amount of wax used. An Omnivac shell or a partial denture without buccal flanges is fabricated as a guide to the amount of distraction required.
Surgical placement of the distractor includes osteotomy and mobilization of the bone transport segment. There is a latency period of 4 to 7 days, depending on the size and location of the transport segment, before the distractor is activated. When activation is begun, the amount of daily activation depends on the size of the segment to be distracted. (The smaller the segment, the less cancellous bone is available and the slower the rate of distraction.) The recommended rate is 0.4 mm, twice a day.
Achievement of the target distraction is confirmed by insertion of the omnivac shell or flangeless denture. The omnivac shell can also be used to establish the papillary form. Overdistraction of 2 to 3 mm is necessary to compensate for relapse. A consolidation period of at least 2 months is required. The greater the amount of distraction performed, the longer the necessary consolidation period.
Case 3: Traumatic loss of six mandibular anterior teeth
A 35-year-old patient was involved in a motor vehicle accident and lost six mandibular anterior teeth and the associated alveolar bone (Fig 3-3a). Iliac crest bone augmentation was attempted but failed because of the lack of soft tissue coverage.
DO using bidirectional distractors was chosen as an alternative to build back the alveolus along with the soft tissue. After the patient was administered general anesthesia, an oscillating scalpel saw was used to make bony cuts and a bidirectional distractor was placed (Figs 3-3b and 3-3c).
Activation commenced after 1 week of latency. The rate of distraction was two half-turns (0.8 mm per day) by the patient at home (Fig 3-3d). After 20 days of activation, a full length of 15.0 mm and sufficient height, level with the alveolar plane, were achieved (Fig 3-3e). The postoperative radiograph revealed the fully activated device (Fig 3-3f).
Horizontal distraction then commenced by clockwise rotation of the nuts, which pulled the bone transport segment facially a distance of 4 mm over a period of several days. An occlusal radiograph was taken to determine the extent of the horizontal movement of the bone transport segment (Fig 3-3g).
The patient was asked to wait 2 months to allow consolidation. After the consolidation period, the 2DCD was removed after the administration of local anesthesia, and five implants were placed in the distracted area (Fig 3-3h). In the area of the mandibular left canine (the area of the vertical bone cut), it was impossible to place an implant, and the patient preferred not to go through another bone graft at this area. Three months later, the area was reconstructed with a porcelain-fused-to-metal fixed partial denture.
Case 3: Traumatic loss of six mandibular anterior teeth
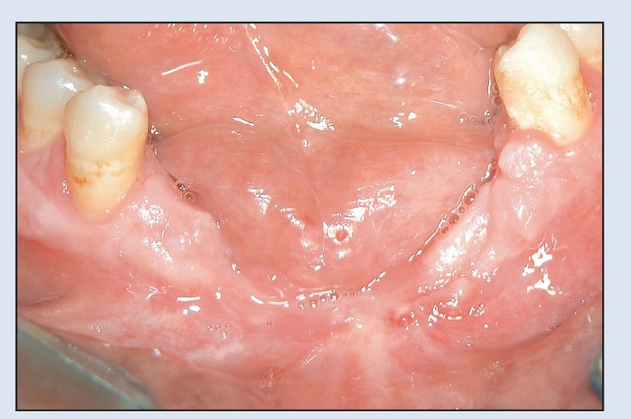
Fig 3-3a The patient experienced complete traumatic loss of the anterior alveolus and teeth.



