Mandibular canines are much less frequently impacted than the maxillary canines.
Most mandibular canines are found in a labial position. But sometimes they can be in the mental protuberance area or lying transversely at the lower border of mandible. They can migrate to the opposite side of the mandible, i.e. transposition of canine (Figs 23.1A and B, 23.2A and B). Such teeth maintain their original innervation and this fact has to be considered when removing them under local anesthesia.
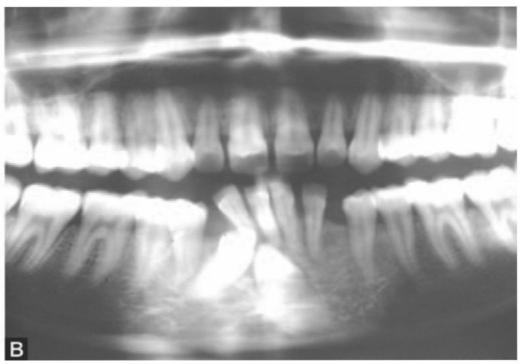
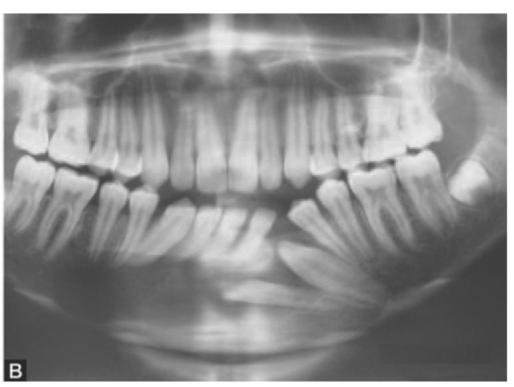
Patients with impacted mandibular canine also presents with symptoms comparable to that of impacted maxillary canine like retained deciduous teeth, proclination/displacement of adjacent incisors (Figs 23.3A and B) or clinical features associated with cyst formation (Figs 23.4A and B). Impacted canines may remain symptom free and are then discovered accidentally in a routine radiograph or while investigating for other diseases (Figs 23.5). It may sometimes lead to recurrent pain and infection (Figs 23.6A and B).
Treatment
The following treatment options should be considered in the management of impacted mandibular canine:
1.Observation: In many cases this modality is acceptable if indications for removal do not exist like impingement on adjacent tooth, development of follicular cyst or as a part of the planned orthodontic
treatment. The retained primary may be permitted to continue for an extended period. However, the impacted tooth should be periodically reviewed to assess the development of pathologic changes.
2.Exposure and orthodontic repositioning: This can be considered if there is adequate space for the accommodation of the tooth in the arch and if the angulation of the tooth is favorable, i.e. deviation of the long axis of the tooth is not excessive. The treatment is carried out in the same manner as for the maxillary canine.
3.Surgical repositioning: This may be considered as an alternative treatment option if exposure and orthodontic repositioning is not possible. The optimal time for surgical repositioning appears to be before the root formation is complete, i.e. when the apical foramen is still wide open. In such cases pulpal revascularization and periodontal healing are very predictable. With further root development, the tooth may require endodontic treatment.
4.Surgical removal of the tooth: The following are the indications for the removal of impacted mandibular canine:
a.Evidence of pathology around the tooth, e.g. follicular cyst, tumor.
b.Close proximity of the follicle to the marginal periodontium of the adjacent tooth.
c.Orthodontic need to move adjacent tooth into the area.

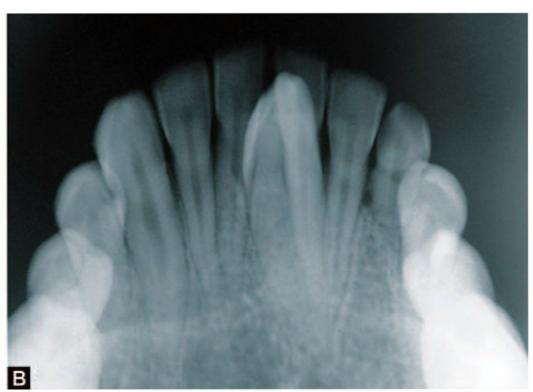
Figs 23.1A and B: Transposition of 33 to the midline. (A) Intraoral view, (B) Occlusal X-ray of the patient

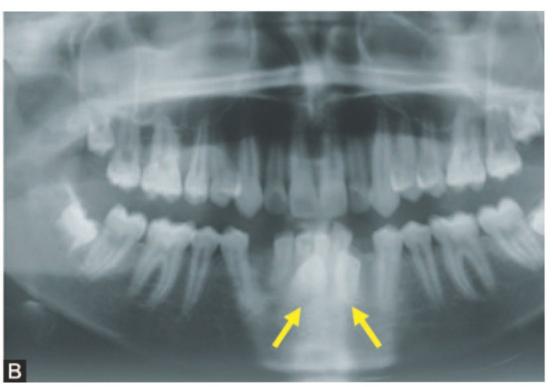
Figs 23.2A and B: Transposition of both lower canines. (A) Clinical appearance of the patient, (B) OPG of the patient showing transposed canines (yellow arrows)

Figs 23.3A and B: Impacted canines causing displacement of lower anterior teeth. (A) Proclination of lower incisor teeth, (B) OPG of the patient showing both lower canines impacted

Figs 23.4A and B: Impacted canine associated with dentigerous cyst of mandible (A) Operative appearance showing impacted canine and incisor associated with cyst, (B) OPG of the same patient showing impacted canine and lateral incisor with radiolucent lesion of mandible
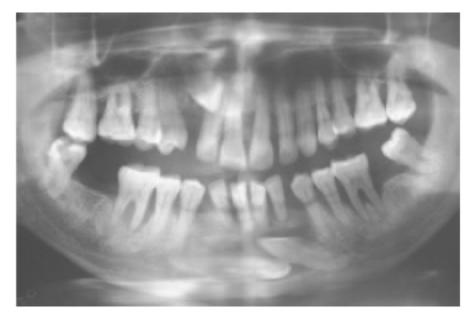
Fig. 23.5: Impacted mandibular canines (bilateral) and impacted right maxillary canine in a 52-year-/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


