Malignant disease
Key Points
• Lifestyle habits underlie several malignant diseases
• Tobacco is responsible for a very wide range of malignant diseases
General Aspects
Malignant neoplasms or ‘cancers’ develop because of deoxyribonucleic acid (DNA) mutations – some spontaneously (possibly due to oxygen radicals), others from chemical carcinogens (e.g. tobacco, alcohol or betel), ionizing and ultraviolet radiation, or oncogenic microorganisms (e.g. hepatitis, herpesviruses and human papillomaviruses (HPVs); Fig. 22.1). Important chemical carcinogens are aromatic amines (including arylamines and heterocyclic amines) found in tobacco smoke and cooked foods. The list of known carcinogens is long; the most important – relevant in tobacco and alcoholic beverages – are shown in Box 22.1.
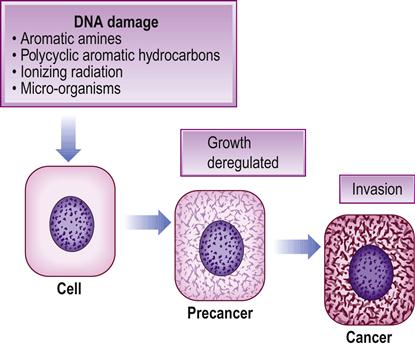
Various liver enzymes termed xenobiotic-metabolizing enzymes (XMEs) are involved in the metabolism of carcinogens or pro-carcinogens (Table 22.1); several are polymorphic and they may be involved in carcinogen activation or degradation. Other enzymes can reverse or repair some of the damage from mutations (DNA repair enzymes) but, when mutations involve genes such as tumour suppressor genes, the cell may become autonomous, despite attempts at DNA and cell repair, and the cell then proliferates and invades – the hallmark of cancer. Eventually, the tumour spreads elsewhere (metastasizes) to lymph nodes and through the blood.
Table 22.1
| Enzyme | Abbreviation | Main activities of some genotypes |
| Alcohol dehydrogenases | ADH | Activate ethanol |
| Aldehyde dehydrogenases | ALDH | Inactivate ethanol |
| Cytochrome P450 | CYP | Activate ethanol, benzpyrene and nitrosamines |
| Glutathione S-transferases | GST | Metabolize benzpyrene, alkyl halides, epoxides and lipid peroxides |
| N-acetyl transferases | NAT | Acetylate arylamines |
Carcinomas are malignant neoplasms that arise from epithelia; they are a leading cause of morbidity and mortality, mainly in persons who are middle-aged or older, and are most common in the lung, breast, colon, cervix, stomach, pancreas, ovary, prostate and skin. They metastasize mainly to the brain, liver and bones.
Oral cancer is discussed below. Lung tumours are discussed in Chapter 15, breast, ovary and prostate cancer in Chapter 25, gastrointestinal and pancreatic cancer in Chapter 7, haematological malignancies in Chapter 8, brain tumours in Chapter 13, liver cancer in Chapter 9 and skin cancer in Chapter 11.
Cancer Prevention
The prognosis of malignant disease is generally poor and unfortunately treatment can also have significant adverse effects, so prevention and early detection are important. The European Code against Cancer summarizes the preventive aspects (Box 22.2). The World Cancer Research Fund advocates measures in addition to not using tobacco and alcohol, and avoiding sun exposure, as in Table 22.2.
Table 22.2
Ten rules for reducing cancer risk
| Rule | Rationale |
| 1. Be as lean as possible without being underweight | Convincing evidence shows that weight gain and obesity increase the risk of cancers, including bowel and breast. Maintain healthy weight through a balanced diet and regular physical activity to keep your risk lower |
| 2. Be physically active for at least 30 min every day | Strong evidence shows that physical activity protects against cancers, including bowel and breast. Being physically active is also key to maintaining a healthy weight |
| 3. Avoid sugary drinks. Limit consumption of energy-dense foods (particularly processed foods high in added sugar, or low in fibre or high in fat) | Energy-dense foods are high in fats and sugars, and often low in nutrients; especially when consumed frequently or in large portions, they increase the risk of obesity, which increases the risk of cancer. Fast foods like burgers, chips, fried chicken and pizzas, and snack foods like chocolate, crisps and biscuits tend to be energy-dense. Some energy-dense foods, such as nuts, seeds and vegetable oils, are important sources of nutrients, and have not been linked with weight gain as part of a typical diet |
| 4. Eat more of a variety of vegetables, fruits, wholegrains and pulses such as beans | Evidence shows that vegetables, fruits and other foods containing dietary fibre (such as wholegrains and pulses) may protect against a range of cancers, including mouth, stomach and bowel. They also help protect against weight gain and obesity. As well as eating five portions a day, try to include wholegrains (e.g. brown rice, wholemeal bread and pasta) and/or pulses with every meal. Sugary drinks, such as colas and fruit squashes, can also contribute to weight gain. Fruit juices, even without added sugar, are likely to have a similar effect. Try to eat less energy-dense foods, such as vegetables, fruits and wholegrains instead. Opt for water or unsweetened tea or coffee in place of sugary drinks |
| 5. Limit consumption of red meats (such as beef, pork and lamb) and avoid processed meats | There is strong evidence that red and processed meats are causes of bowel cancer. Aim to limit intake of red meat to less than 500 g cooked weight (about 700–750 g raw weight) a week. Try to avoid processed meats (bacon, ham, salami, corned beef, sausages) |
| 6. If consumed at all, limit alcoholic drinks to 2 a day for men and 1 a day for women | There is evidence that alcoholic drinks can increase the risk of a number of cancers, including breast and colon. Any alcohol consumption can increase cancer risk. There is some evidence to suggest that small amounts of alcohol can help protect against heart disease. If you choose to drink, do so in moderation |
| 7. Limit consumption of salty foods and food processed with salt (sodium) | Evidence shows that salt and salt-preserved foods probably cause stomach cancer and hypertension. Processed foods, including bread and breakfast cereals, can contain large amounts of salt |
| 8. Do not use supplements to protect against cancer | High-dose nutrient supplements can affect cancer risk, so it is best to opt for a balanced diet without supplements. However, supplements are advisable for some groups of people |
| 9. It is best for mothers to breast-feed exclusively for up to 6 months and then add other liquids and foods | Strong evidence shows that breast-feeding protects mothers against breast cancer and babies from excess weight gain |
| 10. After treatment, cancer survivors should follow the recommendations for cancer prevention | Maintaining a healthy weight through diet and physical activity may help to reduce the risk of cancer recurrence |
Avoidance of Tobacco
Tobacco is best avoided; up to 30% of cancers in developed countries are tobacco-related. Tobacco smoke is a mixture of at least 50 compounds, including polycyclic aromatic hydrocarbons (PAHs), nitrosamines, aldehydes and aromatic amines. Tobacco, acting either singly or jointly with the consumption of alcohol, is responsible for 87% of lung cancer, and between 43% and 60% of cancers in oesophagus, larynx and oral cavity. Tobacco consumption is also linked to cancers of the bladder and pancreas, a minority of cancers of the kidney, stomach, cervix and nose, and myeloid leukaemia. On smoking cessation, the risk of cancer rapidly declines; benefit is evident within 5 years and is progressively greater over time.
Although the greatest cancer hazard is caused by cigarette smoking, cigars can cause similar hazards, and both cigar smoking and pipe smoking are implicated in cancers of the oral cavity, pharynx, larynx and oesophagus. Bidi, a type of cigarette made of tobacco rolled in a dried temburni leaf, is smoked in India and is associated with a high incidence of oral leukoplakia and oral cancer. Tobacco smoke released to the environment by smokers, commonly referred to as environmental tobacco smoke (ETS) and which is responsible for ‘passive smoking’, has several deleterious effects on people who inhale it. It causes a small rise in the risk of lung cancer, and also some increase in the risk of heart disease and respiratory disease. It is particularly harmful to small children.
Tobacco-chewing in peoples from parts of Asia, along with a variety of ingredients in a ‘betel quid’ (betel vine leaf, areca nut, catechu and slaked lime, together with tobacco) appears to predispose to oral squamous cell carcinoma (OSCC). Smokeless tobacco, for example snuff-dipping in women in the south-eastern USA who place snuff in the buccal sulcus, predisposes to gingival and alveolar carcinoma close to where the snuff is placed, but the risk is low.
Avoidance of Alcohol
Alcoholic beverages may contain carcinogens or pro-carcinogens, including ethanol, nitrosamines and urethane contaminants. The total amount of ethanol ingested appears to be the key factor. Alcoholic beverages increase the risk of squamous cell cancers of the oral cavity, pharynx, larynx and oesophagus. Alcohol-drinking raises the risk of neoplasms, even in the absence of smoking, but alcohol-drinking and tobacco-smoking together greatly increase the risk. A probable carcinogenic mechanism of alcohol is the facilitation of the effect of tobacco and possibly of other carcinogens to which the upper digestive and respiratory tracts are exposed, particularly those of dietary origin. However, a direct carcinogenic effect of acetaldehyde, the main metabolite of ethanol, and of other agents present in alcoholic beverages, is likely. A diet poor in fruits and vegetables, typical of heavy drinkers, may also play a role.
Alcohol-drinking is also strongly associated with the risk of primary liver cancer, particularly among smokers and among people chronically infected with hepatitis C virus. A higher risk of colorectal cancer seems to be linearly correlated with the amount of alcohol consumed and independent of the type of alcohol. A greater risk of breast cancer has been consistently reported. More cases of breast cancer than of any other cancer are attributable to alcohol-drinking among European women. It has been suggested that alcohol acts on hormonal factors involved in breast carcinogenesis.
Few studies have analysed the relation between stopping alcohol-drinking and the risk of cancers of the upper respiratory and digestive tracts, but there is clear evidence that the risk of oesophageal cancer falls by 60%, 10 years or more after drinking cessation.
Other Factors
Weight reduction
Obesity is associated with a greater risk of cancer of the colon, breast (post-menopausal), endometrium, kidney and oesophagus (adenocarcinoma). In Western Europe, it has been estimated that being overweight or obese accounts for approximately 11% of all colon and breast cancers, 39% of endometrial cancers, 27% of oesophageal adenocarcinomas and 25% of renal cell cancers. A body mass index of below 25 kg/m2 should, if possible, be maintained.
Greater physical activity
There is consistent evidence that regular physical activity is associated with a 40% reduction in the risk of colorectal, breast and oesophageal cancer and may possibly also lower the risk of prostate cancer. The protective effect of physical activity improves with increasing levels of activity. One hour per day of moderate physical activity, such as walking, may also be needed to maintain a healthy body weight, particularly for people with sedentary lifestyles.
Greater intake of fruit and vegetables
A low-fat diet with at least 11 servings of fruits, vegetables, wholegrains and beans daily may reduce the chances of colon cancer by 75%, breast cancer by 50% and lung cancer by 30%. There may also be a protective effect on the risk of a wide variety of other cancers, in particular oral, oesophagus, stomach, rectum and pancreas.
‘Five-a-day’ (minimum 400 g/day, i.e. two pieces of fruit and 200 g of vegetables) is advocated to lead to a lower cancer risk. Vegetables and fruits contain many potentially anticarcinogenic agents. Antioxidant activity seems important in cancer protection but the exact molecule(s) in vegetables and fruits that confer(s) protection is/are unknown and the mechanism of action unclear.
Avoidance of sun exposure
Ninety per cent of skin cancers are seen in white-skinned peoples and are caused by the sun’s ultraviolet rays (Ch. 11). Squamous cell carcinoma of the skin or lip shows the clearest relationship with sun exposure and the risk is greatest in outdoor workers. The recipients of transplanted organs are particularly at risk as a result of the combined effects of the unchecked growth of human papillomavirus (HPV) due to immunosuppression, and exposure to the sun (Ch. 35).
Malignant melanoma is more common in people of high socioeconomic status who work inside but who have the opportunity to spend leisure time in the sun, and this includes dentists. The incidence of melanoma has doubled in Europe in 30 years, and this is attributed to longer intense sun exposure. The fair-skinned are more susceptible, particularly those with red hair, freckles and a tendency to burn in the sun. These characteristics are genetically determined at least partially by the MCIR gene, which codes for the melanocyte-stimulating hormone receptor. Variants in the MCIR gene control the ratio of black melanin (eumelanin) to red (phaeomelanin) in the skin. The strongest phenotypic risk factor for melanoma, however, is the presence of large numbers of moles or melanocytic naevi, which may be normal in appearance but are also usually accompanied by so-called atypical moles. The latter are larger than 5 mm in diameter with variable colour and an irregular shape. The phenotype, described as the atypical mole syndrome (AMS) phenotype, is present in around 2% of the Caucasian population and is associated with an approximately tenfold higher risk of melanoma. Advice on sun protection is of particular importance to this population.
The best protection from the summer sun is to stay out of it. If outdoors, keep out of the sun between 11.00 a.m. and 3.00 p.m., wear close-weave heavy cotton and use sunscreens with high sun protection factor (SPF). Do not rely upon sunscreens for protection.
Avoidance of occupational exposures
The cancers that have most frequently been associated with occupational exposures are those of the lung, urinary bladder, mesothelioma, larynx, liver, nose and nasal cavity, and skin, as well as leukaemia (non-melanoma). The more common occupational exposures are solar radiation, passive smoking, crystalline silica, diesel exhaust, radon, wood dust, benzene, asbestos, formaldehyde, PAHs, chromium, cadmium and nickel compounds. There is no reliable evidence of a risk from power plants, power lines or mobile telephones.
Many chemicals are known or suspected carcinogens. Many are still widely used: for example, 1,3-butadiene and formaldehyde. Prevention of workplace exposures can be effective; the incidence of occupational bladder cancer fell after the ban on the use of beta-naphthylamine in the rubber and chemical industries.
Avoidance of environmental exposures
The term ‘environmental exposures’ usually refers to exposures of the general population that cannot be directly controlled by the individual; these include air pollution, drinking water contaminants, passive smoking, radon gas in buildings, exposure to solar radiation, food contaminants such as pesticide residues, dioxins or environmental oestrogens, chemicals from industrial emissions, ionizing radiation, waste from nuclear processes, and others. These exposures have been associated with cancers of the lung, urinary bladder, leukaemia and skin. The impact of several exposures that are widespread, such as disinfection by-products in drinking water, is still inconclusive. Agents in the general environment to which many are exposed for long periods (such as passive smoking or air pollution) may increase the relative risk for certain cancers only modestly, but may be responsible for a significant number of cases overall.
Avoidance of hormones that may play a role
Hormone replacement therapy (HRT) for menopausal symptoms appears to raise the risk of breast cancer.
Cancer Screening
Table 22.3 shows cancer screening methods.
Table 22.3
| Cancer site | Methods |
| Breast | Self-examination/mammography/BRCA1 and BRAC2 mutation in Jewish women |
| Cervix | Cervical cytology/human papillomavirus testing |
| Colon/rectum | Faecal occult blood/flexible sigmoidoscopy |
| Lung | Spiral computed tomography (CT) or chest radiography |
| Neuroblastoma | Urinary homovanillic acid (HVA) and vanillylmandelic acid (VMA) |
| Oral | Examination of the mouth |
| Ovary | Cancer antigen 125 (CA125) and/or ultrasonography |
| Prostate | Prostate-specific antigen (PSA) |
| Skin (melanoma) | Examination for moles |
| Stomach | Helicobacter pylori testing; breath test/endoscopy |
| Testis | Self-examination |
Clinical Features
There is a range of different cancers (Box 22.3), each with specific manifestations (see relevant chapters). Features that may raise suspicion of cancer are shown in Box 22.4.
Management
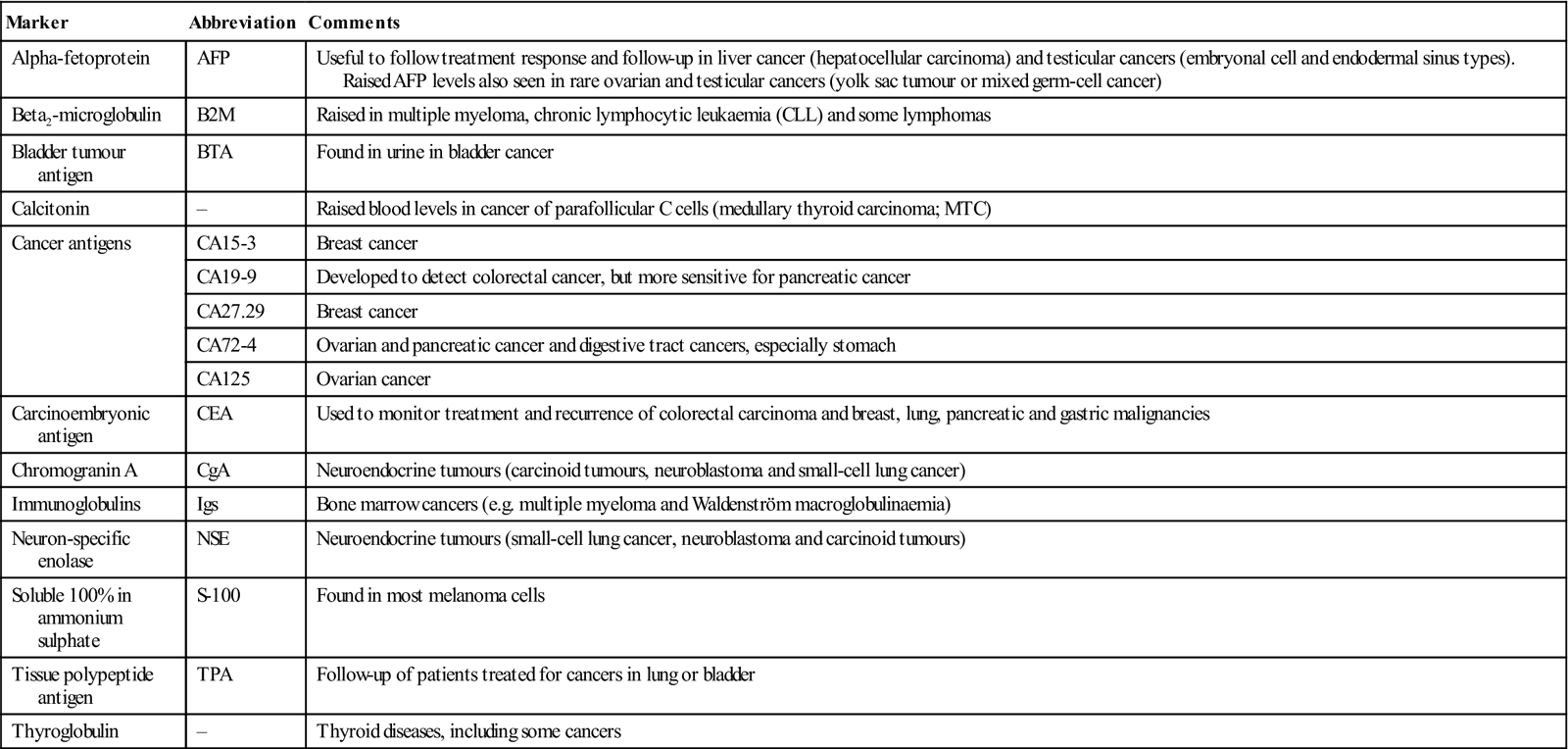
Clinical examination, supplemented with imaging and biopsy, is invariably indicated to diagnose malignant disease. There is also considerable interest in tumour markers in blood or other body fluids, or in tissues; unfortunately, none of these tumour markers, including carcinoembryonic antigen (CEA), meets the goal of reliably finding cancer at an early stage. Because of this, ‘tumour markers’ are used mainly in patients who have already been diagnosed with cancer in order to monitor treatment response or detect recurrences. The most widely accepted tumour marker assessment is the prostate-specific antigen (PSA) blood test, which is used (along with the digital rectal examination) to screen for prostate cancer; it also suffers from the drawbacks outlined in Chapter 25. Others tumour markers are shown in Table 22.4.
Table 22.4
< ?comst?>
| Marker | Abbreviation | Comments |
| Alpha-fetoprotein | AFP | Useful to follow treatment response and follow-up in liver cancer (hepatocellular carcinoma) and testicular cancers (embryonal cell and endodermal sinus types). Raised AFP levels also seen in rare ovarian and testicular cancers (yolk sac tumour or mixed germ-cell cancer) |
| Beta2-microglobulin | B2M | Raised in multiple myeloma, chronic lymphocytic leukaemia (CLL) and some lymphomas |
| Bladder tumour antigen | BTA | Found in urine in bladder cancer |
| Calcitonin | – | Raised blood levels in cancer of parafollicular C cells (medullary thyroid carcinoma; MTC) |
| Cancer antigens | CA15-3 | Breast cancer |
| CA19-9 | Developed to detect colorectal cancer, but more sensitive for pancreatic cancer | |
| CA27.29 | Breast cancer | |
| CA72-4 | Ovarian and pancreatic cancer and digestive tract cancers, especially stomach | |
| CA125 | Ovarian cancer | |
| Carcinoembryonic antigen | CEA | Used to monitor treatment and recurrence of colorectal carcinoma and breast, lung, pancreatic and gastric malignancies |
| Chromogranin A | CgA | Neuroendocrine tumours (carcinoid tumours, neuroblastoma and small-cell lung cancer) |
| Immunoglobulins | Igs | Bone marrow cancers (e.g. multiple myeloma and Waldenström macroglobulinaemia) |
| Neuron-specific enolase | NSE | Neuroendocrine tumours (small-cell lung cancer, neuroblastoma and carcinoid tumours) |
| Soluble 100% in ammonium sulphate | S-100 | Found in most melanoma cells |
| Tissue polypeptide antigen | TPA | Follow-up of patients treated for cancers in lung or bladder |
| Thyroglobulin | – | Thyroid diseases, including some cancers |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Surgery, radiotherapy and chemotherapy are the main treatments for cancer.
Oral Cancer
General Aspects
Oral cancer is usually squamous cell carcinoma (OSCC) and is the predominant cancer in the head and neck. It is mainly a disease of older males. High rates of OSCC are seen particularly in India, Sri Lanka, Brazil, Hungary and France, and there is a wide geographical variation in incidence. Risk factors are shown in Box 22.5. The results of many studies of lifestyle risk factors have been summarized by the International Agency for Research on Cancer (IARC) and show the importance of specific factors (i.e. tobacco, betel and alcohol use).
Tobacco contains a number of addictive components, especially nicotine, and releases many carcinogens (see above). Tobacco use in all forms appears to carry a risk of OSCC. Oral cancer risks show a clear decline after stopping tobacco use. Snuff – finely powdered plant material, principally tobacco, used orally or nasally – is a risk factor for OSCC.
Betel quid (BQ) is probably used by 20% of the world’s population and may lead to:
Increased consumption of alcohol-containing beverages is associated with a risk of OSCC. The risk decreases after stopping alcohol use but the effects appear to persist for several years. The type of alcoholic beverage appears to influence the risk – hard liquors conferring higher risks. There have been reports of oral cancer in marijuana smokers and in users of alcohol-containing mouthwashes but any relationships have yet to be confirmed by full epidemiological studies.
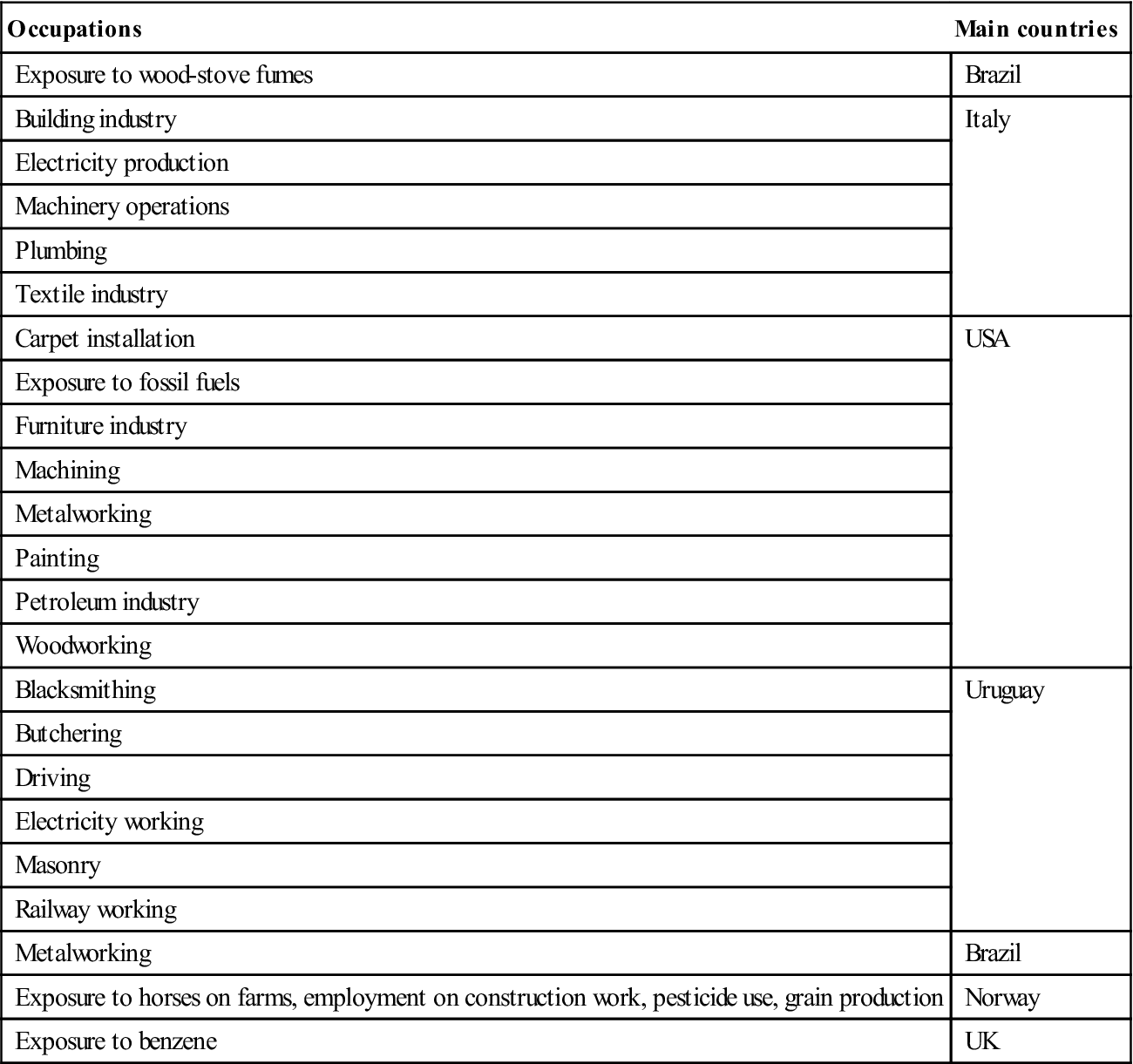
Charcoal-grilled red meat and fried foods have been implicated as risk factors, but an increased consumption of fruits and vegetables is associated with lower risk of OSCC. Higher risks of oral cancer have also been found in a number of occupations (Table 22.5).
Table 22.5
Occupations associated with risk of oral cancer
< ?comst?>
| Occupations | Main countries |
| Exposure to wood-stove fumes | Brazil |
| Building industry | Italy |
| Electricity production | |
| Machinery operations | |
| Plumbing | |
| Textile industry | |
| Carpet installation | USA |
| Exposure to fossil fuels | |
| Furniture industry | |
| Machining | |
| Metalworking | |
| Painting | |
| Petroleum industry | |
| Woodworking | |
| Blacksmithing | Uruguay |
| Butchering | |
| Driving | |
| Electricity working | |
| Masonry | |
| Railway working | |
| Metalworking | Brazil |
| Exposure to horses on farms, employment on construction work, pesticide use, grain production | Norway |
| Exposure to benzene | UK |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Microorganisms implicated in the aetiology of OSCC include syphilis, Candida albicans and viruses such as herpesviruses and HPV. Syphilis is discussed in Chapter 32. Candidal leukoplakias are potentially malignant and autoimmune polyendocrinopathy–candidiasis–ectodermal dystrophy (APECED), an autosomal recessive disease associated with a limited T-lymphocyte defect, seems to favour the growth of C. albicans and predisposes to OSCC. Viral infections, particularly with oncogenic HPV subtypes and possibly Epstein–Barr virus (EBV), can have a tumorigenic effect. Oropharyngeal cancer is significantly associated with oral HPV and also with a high lifetime number of vaginal-sex partners and oral-sex partners; HPV-16 DNA is detected in most.
Lip cancer is seen mainly in males with chronic sun exposure and in smokers. Antihypertensive agents increase the risk. Ionizing radiation exposure is a possible risk factor for second primary cancers. Persons with poor oral hygiene appear to have an increased risk of OSCC, independent of any effect of tobacco, alcohol, or other well-proven risk factors; not all workers agree, however, so further studies are required. Polymicrobial supragingival plaque is a possible independent factor, as it possesses a relevant mutagenic interaction with saliva, and individual oral health is a cofactor in the development of OSCC. Viridans group streptococci of the normal oral flora can produce acetaldehyde in vitro during ethanol incubation via alcohol dehydrogenase. In particular, the clinical strain of Streptococcus salivarius, both clinical and culture collection strains of Streptococcus intermedius and the culture collection strain of Streptococcus mitis produced high amounts of acetaldehyde.
Systemic Health and Oral Squamous Cell Carcinoma
There is a highly significant increase in the incidence of OSCC in dyskeratosis congenita and systemic sclerosis, and an increase of potentially malignant lesions and OSCC in transplant recipients and in people with cancers elsewhere in the upper aerodigestive tract. There is a putative association of diabetes mellitus with oral cancer.
Potentially Malignant Disorders
Some potentially malignant (pre-cancerous) oral clinical lesions that can progress to OSCC include the following, in particular:
■ erythroplasia (erythroplakia) – the most likely lesion to progress to severe dysplasia or carcinoma
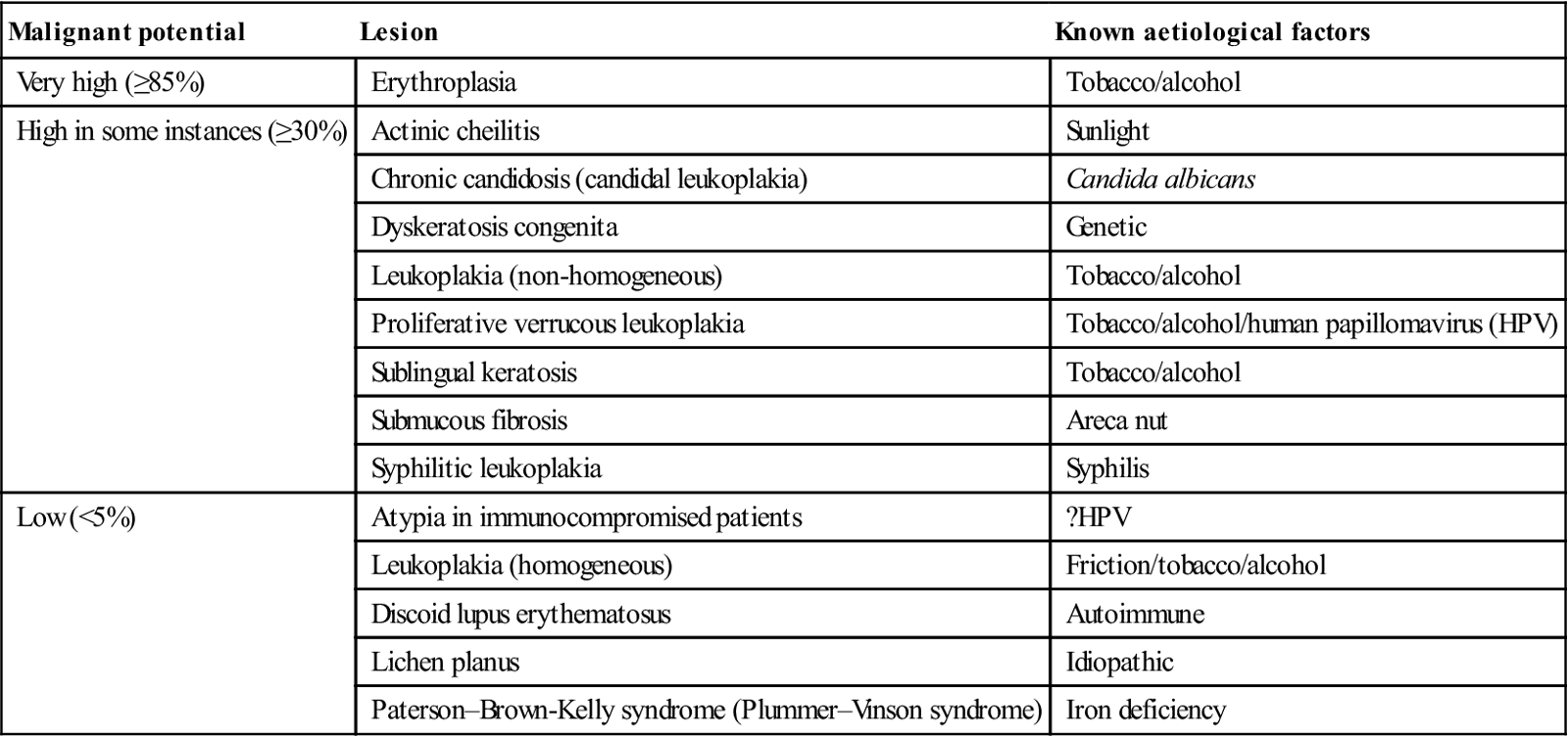
Apart from these lesions, most other potentially malignant lesions or conditions have only a very low incidence of dysplasia or malignant change (Table 22.6).
Table 22.6
Potentially malignant oral disorders
< ?comst?>
| Malignant potential | Lesion | Known aetiological factors |
| Very high (≥85%) | Erythroplasia | Tobacco/alcohol |
| High in some instances (≥30%) | Actinic cheilitis | Sunlight |
| Chronic candidosis (candidal leukoplakia) | Candida albicans | |
| Dyskeratosis congenita | Genetic | |
| Leukoplakia (non-homogeneous) | Tobacco/alcohol | |
| Proliferative verrucous leukoplakia | Tobacco/alcohol/human papillomavirus (HPV) | |
| Sublingual keratosis | Tobacco/alcohol | |
| Submucous fibrosis | Areca nut | |
| Syphilitic leukoplakia | Syphilis | |
| Low (<5%) | Atypia in immunocompromised patients | ?HPV |
| Leukoplakia (homogeneous) | Friction/tobacco/alcohol | |
| Discoid lupus erythematosus | Autoimmune | |
| Lichen planus | Idiopathic | |
| Paterson–Brown-Kelly syndrome (Plummer–Vinson syndrome) | Iron deficiency |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Clinical Features
Common sites for OSCC are the lips, the lateral border of the tongue, and the floor of the mouth. There may be widespread dysplastic mucosa (‘field change’) or even a second primary neoplasm anywhere in the oral cavity, oropharynx or upper aerodigestive tract.
Cancer must be suspected, especially when there is a single oral lesion persisting for more than 3 weeks, and particularly when having the features shown in Box 22.6. Many OSCCs can be detected visually but early OSCC can be asymptomatic, may appear innocuous and can be overlooked, especially if the examination is not thorough. The whole oral mucosa should be examined, often along with the rest of the upper aerodigestive tract – and the cervical lymph nodes must always be carefully examined by palpation (Fig. 22.2). Various stains or lights purported to help diagnosis tend to lack sensitivity or specificity. Biopsy is invariably indicated.
Classification/Grading
Oral cancer is a term that usually includes cancer of the lip, tongue, salivary glands and other sites in the mouth (gum, floor of the mouth and other unspecified parts of the mouth). Pharyngeal cancer is a term that includes cancers of the nasopharynx, oropharynx and hypopharynx.
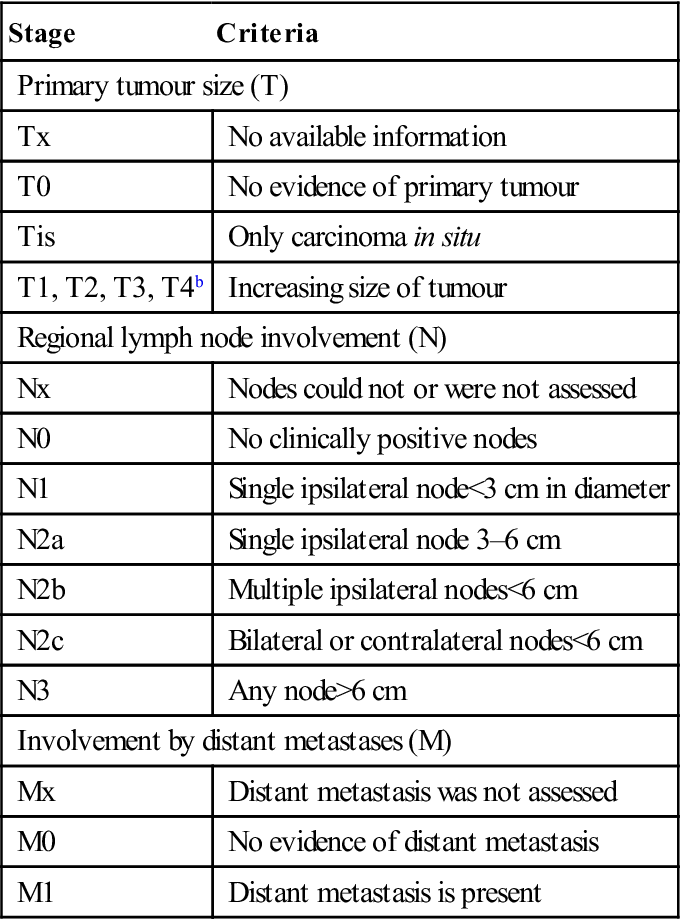
Staging of OSCC should be made according to the TNM classification of the International Union against Cancer (UICC) – tumour size (T), nodal metastases (N) and distant metastases (M; Table 22.7) – since this classification relates well to overall survival rate (i.e. the earlier the tumour is detected, the better the prognosis and the less complicated the treatment).
Table 22.7
TNM classification of malignant neoplasmsa
< ?comst?>
| Stage | Criteria |
| Primary tumour size (T) | |
| Tx | No available information |
| T0 | No evidence of primary tumour |
| Tis | Only carcinoma in situ |
| T1, T2, T3, T4b | Increasing size of tumour |
| Regional lymph node involvement (N) | |
| Nx | Nodes could not or were not assessed |
| N0 | No clinically positive nodes |
| N1 | Single ipsilateral node<3 cm in diameter |
| N2a | Single ipsilateral node 3–6 cm |
| N2b | Multiple ipsilateral nodes<6 cm |
| N2c | Bilateral or contralateral nodes<6 cm |
| N3 | Any node>6 cm |
| Involvement by distant metastases (M) | |
| Mx | Distant metastasis was not assessed |
| M0 | No evidence of distant metastasis |
| M1 | Distant metastasis is present |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
aSeveral other classifications are available, e.g. STNM (S=site).
It is generally accepted that prognosis is best in early carcinomas, especially those that are well differentiated and not metastasized (Table 22.8).
Table 22.8
Prognosis for intraoral carcinoma
| Stage | TNM | Approximate 5-year survival (%) |
| I | T1 N0 M0 | 85 |
| II | T2 N0 M0 | 65 |
| III | /> |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


