
The conventional treatment option for impacted canine is exposure and orthodontic alignment.
Factors’ influencing the prognosis-The prognosis for alignment is dependent on a number of factors which include the age of the patient, spacing/ crowding and the vertical, anteroposterior, and transverse position of the canine crown and root. If the inclination of the canine in relation to the midline is greater than 45 degrees then the prognosis for alignment worsens. The closer the tooth is to the midline the poorer the prognosis. For successful alignment, the root should be neither ankylosed nor dilacerated. The further the canine needs to be moved, the poorer the prognosis for a successful outcome. Similarly as with all orthodontic treatment cooperation and motivation of the patient is supreme. The general dental health should be excellent since the treatment time in these cases is often prolonged. It is generally agreed that the optimum time for alignment is adolescence.
As for any surgical procedure, proper history of the patient should be taken, including the general medical history.
Local examination should emphasize on any bulge labially or palatally, which might give a clue to the position of the tooth.
Radiographs are taken to confirm the position of the impacted tooth and its relationship to the adjacent teeth. Necessary hematological examinations should be done prior to anesthetic assessment.
Choice of anesthesia: Local anesthesia is sufficient in almost all cases of this minor surgical procedure and is
the safest in dental outpatient setting. However, with the change in the social set up, changing out looks of the patient as well as the surgeon and the availability of modern equipments, medicines and techniques general anesthesia has become more popular than earlier times. Another choice is local anesthesia supplemented with intravenous sedation but requires monitoring facilities.
PROCEDURE
a. Palatally positioned canine
The position of the crown of the tooth is determined with the help of radiographs, and a cruciform incision is made with its center over the estimated position of the crown of the buried tooth. The flaps (on four sides) are raised to expose the tooth crown. And once completely exposed, the flaps are excised. Resultant hemorrhage can usually be controlled by pressure. The bone over and surrounding the crown of the tooth is removed in such a way that the crown will be left lying in a saucer-shaped bony cavity, without any sharp ledge of bone at the edges. A pack is inserted to prevent the soft tissues growing over the exposed tooth. The pack can be perio pack or roller gauze impregnated with iodoform or antibiotics, which can be sutured into place (Figs 19.1A to 19.21).
Surgical exposure of palatally impacted canine by excision of overlying mucoperiosteum (Figs 19.2 A to I):
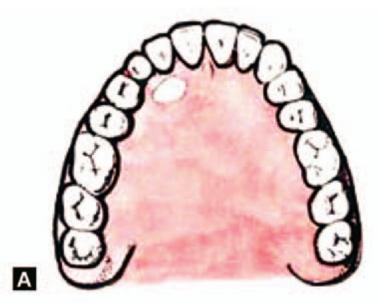
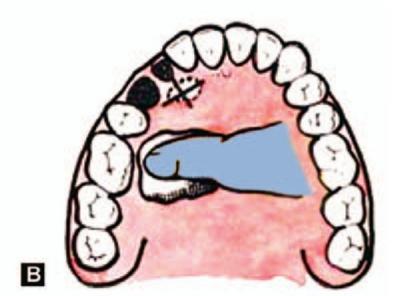
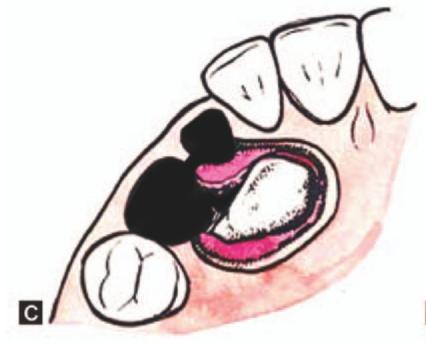
Case report: A 12-year-old girl reported with complaints of unerupted right upper canine and excessive spacing of upper anterior teeth. Intraoral examination showed retained deciduous right upper canine and impacted upper permanent canine (13) and missing upper laterals (Figs 19.2A and B). Periapical X-ray showed that impacted 13 is in a favorable position for orthodontic eruption (Fig. 19.2C). Under local anesthesia, excision of the overlying mucoperiosteum was done to expose the impacted 13 (Figs 19.2D and E). Retained deciduous canine was also extracted (Fig. 19.2F). Zinc oxide eugenol pack was placed to cover the raw area (Fig. 19.2G). After 10 days when the healing has completed, brackets were fixed to the maxillary teeth (Fig. 19.2H). Arch wire was then applied to the maxillary arch and impacted 13 connected to arch wire (Fig. 19.2 I).
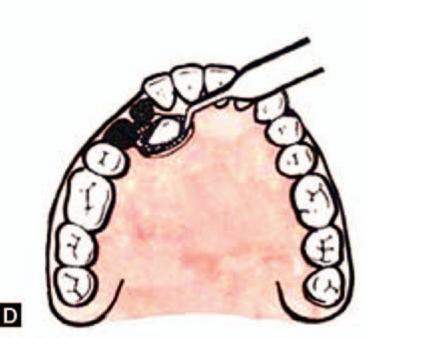
Figs 19.1A to D: Schematic diagram showing exposure of impacted canine in the palate. (A) Position of the crown of the canine is localized by clinical examination and with the help of radiographs, (B) Incision, (C) Excision of the overlying flap and exposure of the crown, (D) Debridement and insertion of the pack
Surgical exposure of palatally impacted canine by creating a window (Figs 19.3 A to I):
In cases where the crown of the tooth cannot be localized, the palatal mucoperiosteal flap is reflected from premolar on the involved side to the canine on the other side, after placing an incision around the neck of the teeth. The crown of the impacted tooth is then exposed by removal of sufficient amount of bone. The part of the mucoperiosteum overlying the crown is excised with a scalpel. The flap is then repositioned and sutured back into place. A pack is placed as explained before (Figs 19.3 A to I).
b. Labially positioned canines
Depending upon the depth and position of the impacted tooth anyone of the following three methods can be employed to expose the crown:
•Creating a surgical window/Gingivectomy
•Closed eruption technique
•Apically positioned flap

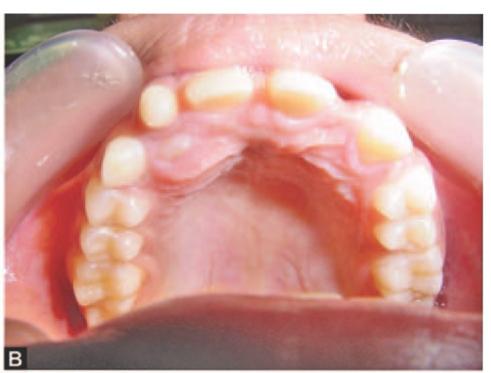


Figs 19.2 A to D: (A) Intraoral view of the patient showing retained deciduous right upper canine, impacted permanent canine (13) and missing upper laterals, (B) Palatal view showing bulge of impacted 13, (C) Periapical X-ray showing impacted 13, (D) Incision marked to expose impacted 13
A. Creating a surgical window/Gingivectomy (Figs 19.4 A to C): If the tooth is situated just beneath the gingiva, simple excision of the overlying soft tissue is enough to expose the crown.
A surgical window or gingivectomy is suggested for shallow, labially positioned maxillary canine impactions close to the alveolar crest or when a broad band of keratinized tissue is present. Implementing the window approach involves resecting a full thickness flap and then repositioning the flap back with a fenestration being opened in the area of the crown. The tooth may erupt normally once the soft tissue obstruction is removed, and in such instances orthodontic treatment may not be required. A gingivectomy procedure is indicated when one half to 2/3 of the crown can be uncovered leaving at least 3 mm of gingival collar. In most instances, the tip of the impacted tooth is near the cemento-enamel junction of the adjacent tooth. This technique is simple but it sacrifices attached gingiva (Kokich et al, 1993).1
B. Closed eruption technique (Figs19.5AtoF): A closed eruption technique is indicated if the tooth is impacted in the middle of the alveolus, near the nasal spine, high in the vestibule or in the palate (Vermette et al, 1995).2 A flap is first reflected over the area of the impacted tooth (Fig. 19.5B). The crown is then exposed (Fig. 19.5C) after removal of the overlying bone if necessary. An orthodontic bracket is bonded to it. A traction wire is connected to the bracket. The flap is closed over the crown, exposing only the traction wire to the oral cavity (Fig. 19.5D). Adequate time is given for the initial healing of the flap. Later the traction wire is connected to an arch wire and optimal force needed to erupt the impacted tooth is exerted (Fig. 19.5E). Figure 19.5F shows the final position of the canine in the arch. Disadvantages of this technique include that once the flap is closed, direct inspection of the tooth is impossible. Moreover, it is difficult to isolate the area and studies have shown a longer eruption time compared to procedures used in open techniques.



Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


