CHAPTER 18
Esthetically Driven Surgical and Prosthetic Management of Alveolar Distraction Osteogenesis
What is now proved was once only imagined.
—William Blake
Restoration of the partially edentulous maxilla with advanced vertical and horizontal deficiencies is a significant multidisciplinary challenge. The objectives of rehabilitation are at the same time both functional and esthetic. They should involve a realistic morphologic duplication of the original elements of the dentofacial complex and the restoration of harmonious relationships between those elements.1,2 The treatment should address osseous, dental, and implant-mucosal deficiencies. Esthetically driven objectives accomplished within sound biologic parameters should provide for the most predictable and stable treatment outcome.3
The initial concern is to establish a stable osseomucosal unit as the foundation for the implant- or tooth-borne prosthesis. Among the available surgical augmentation techniques (autogenous or synthetic bone; connective tissue or soft tissue grafts), most have shortcomings, thus frustrating restorative strategies with postoperative vertical, horizontal, and soft tissue deficiencies. These defects necessitate the utilization of long, esthetically compromised restorations, often modified with pink porcelain or short, unnaturally square teeth, when the dimension of grafted bone or connective tissue is excessive.
Jensen et al4 have confirmed that distraction osteogenesis within the osteoperiosteal flap is the most predictable of the grafting techniques designed to address the complex esthetic and functional deficiencies associated with severe anterior maxillary alveolar atrophy (see chapter 3). They reported the cases of 28 patients with anterior maxillary defects averaging 6.5 mm vertically and 2.0 mm horizontally. A restorative outcome index, scaled from 1 to 10, was tabulated for each case; in the scale, 1 was an extremely poor result, and 10 was a superlative esthetic result. Evaluations over the course of the study rated none of the results as superlative, but 16 of 25 were rated good esthetic outcomes.
Contributing to less than superlative results was a tendency for the osseomucosal segment to distract and heal asymmetrically, particularly horizontally. With the development of improved, bidirectional distraction elements, the ability to accurately position the maxillary osseomucosal segment has improved significantly, thus providing for more predictable osseomucosal segment positioning.5
The attendant prosthetic challenges are to provide a method to precisely locate the transported segment to a prescribed, preplanned, esthetically driven treatment position and to overcome traditional implant prosthetics–related problems of unstable postsurgical soft tissue levels and unpredictable gingival esthetics.
Proposed, in case report format, is an esthetically driven, staged prosthetic-surgical technique in which a series of custom provisional restorations are utilized as surgical guides for initially positioning the transported osseomucosal segment. These custom restorations are then used secondarily to surgically retrofit the definitive prosthesis to a precise, esthetically predetermined treatment position.
 Case Report
Case Report
Case 1: Maxillary anterior edentulism coupled with severe alveolar atrophy and scar tissue
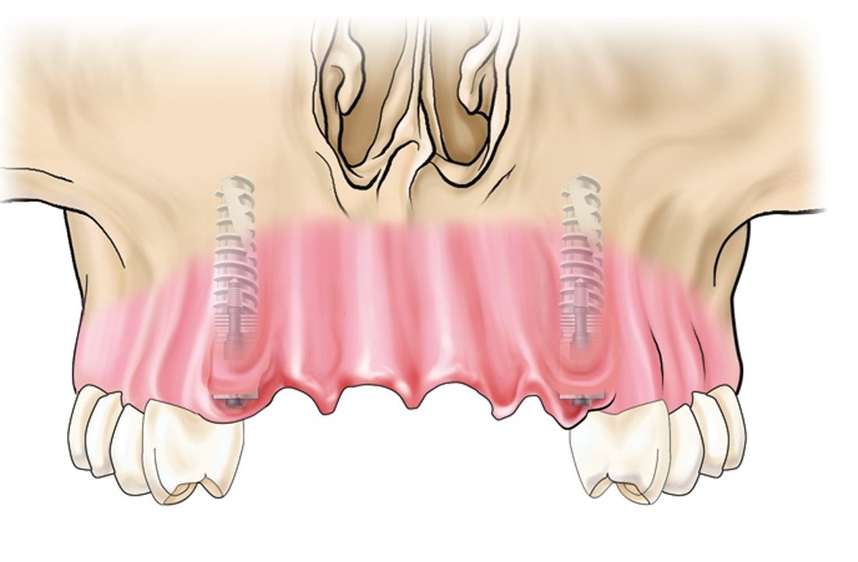
Presented is a challenging case of maxillary partial edentulism (canine to canine) complicated by severe, traumatically induced alveolar atrophy, failed conventional block graft and allograft attempts, and resultant implant failures. The ultimate surgical removal of (1) residual, fragmented expanded polytetrafluoroethylene barrier membrane, (2) residual allograft, and (3) malpositioned implants resulted in marked horizontal (9-mm) and vertical (11-mm) defects, irregular alveolar bone morphology, and significant soft tissue scarring (Fig 18-1). The described treatment approach is a staged, guided distraction osteogenesis within the osteoperiosteal flap, subsequently restored with an implant-supported prosthesis. The procedures are guided by a series of carefully executed provisional prostheses and surgical guides based on those prostheses (Box 18-1).
Box 18-1 Key components of esthetically driven surgical-prosthetic management of alveolar distraction osteogenesis
Stage 1: Distraction
- Fixed provisional prosthesis (FPP)
- Esthetic control cast (ECC)
Stage 2: Implant placement
- Implant surgical guide
- Implant-supported screw-retained provisional prosthesis
Stage 3: Retrofit provisional prosthesis
- Retrofit provisional (RFP) prosthesis
- Cosmetic surgical guide
Stage 4: Definitive prosthesis
- Custom implant abutments and prosthesis framework
Case 1: Maxillary anterior edentulism coupled with severe alveolar atrophy and scar tissue

Fig 18-1a A preoperative smile analysis reveals a narrow arch form with a vertical incisor display.

Fig 18-1b Preoperative maxillary removable partial denture.

Fig 18-1c Prior to surgical intervention, the ridge is loose and mobile but positioned near the alveolar plane.
Fig 18-1d Subsequent to the initial surgical interventions, maxillary anterior vertical bone has been lost.
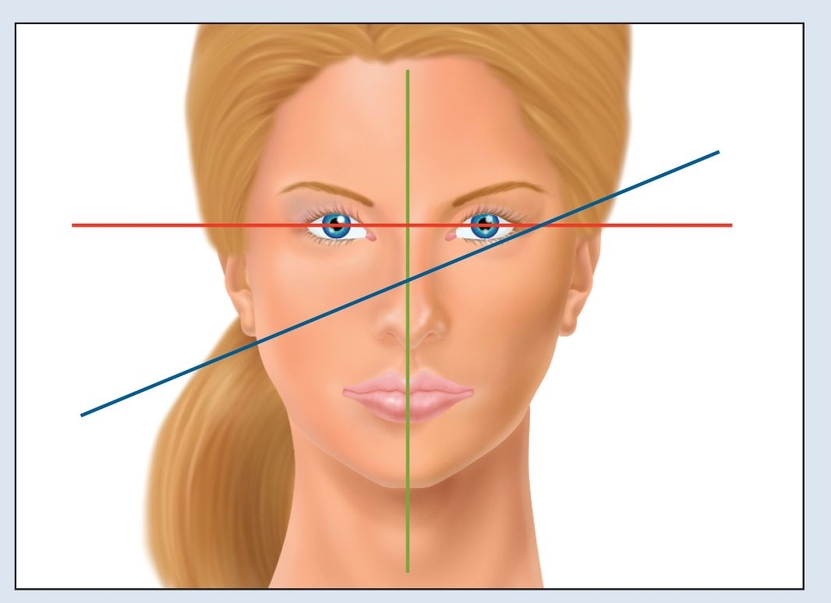
Fig 18-2a The interpupillary line (red), rather than the anatomic position (blue), should be used as a basis for establishing the occlusal plane and incisor position.
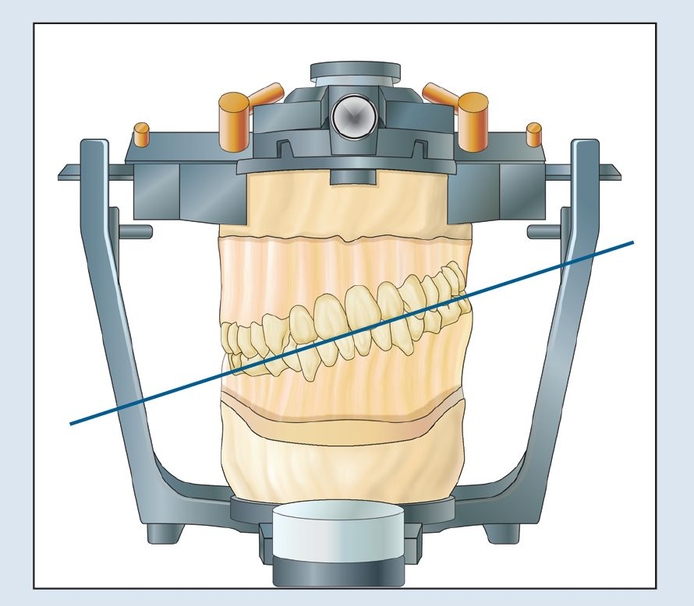
Fig 18-2b A strictly anatomic position (blue line) can lead to a canted maxillary mounting.
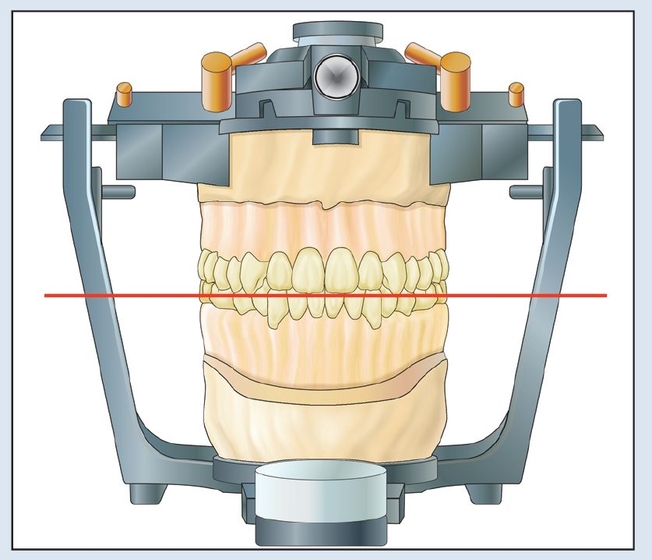
Fig 18-2c Use of the interpupillary line (red) as the landmark establishes the first step toward esthetic management and is termed the esthetic mounting.
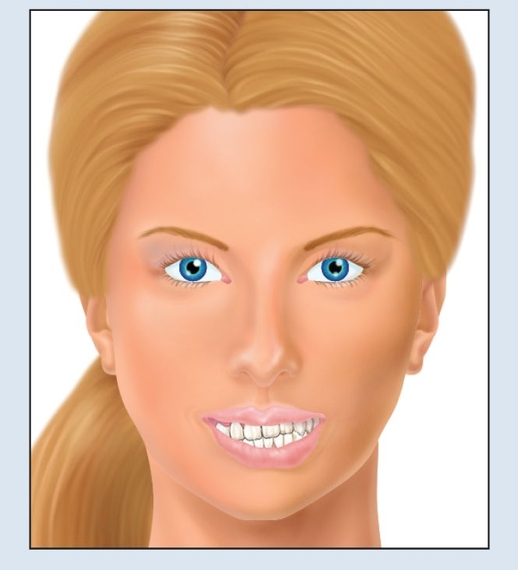
Fig 18-2d Without this approach, the original asymmetry will be replicated in the final restoration.
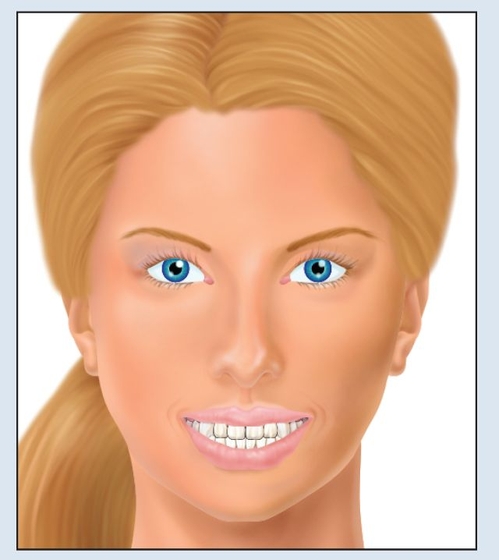
Fig 18-2e With the use of esthetic mounting, facial balance will be obtained.
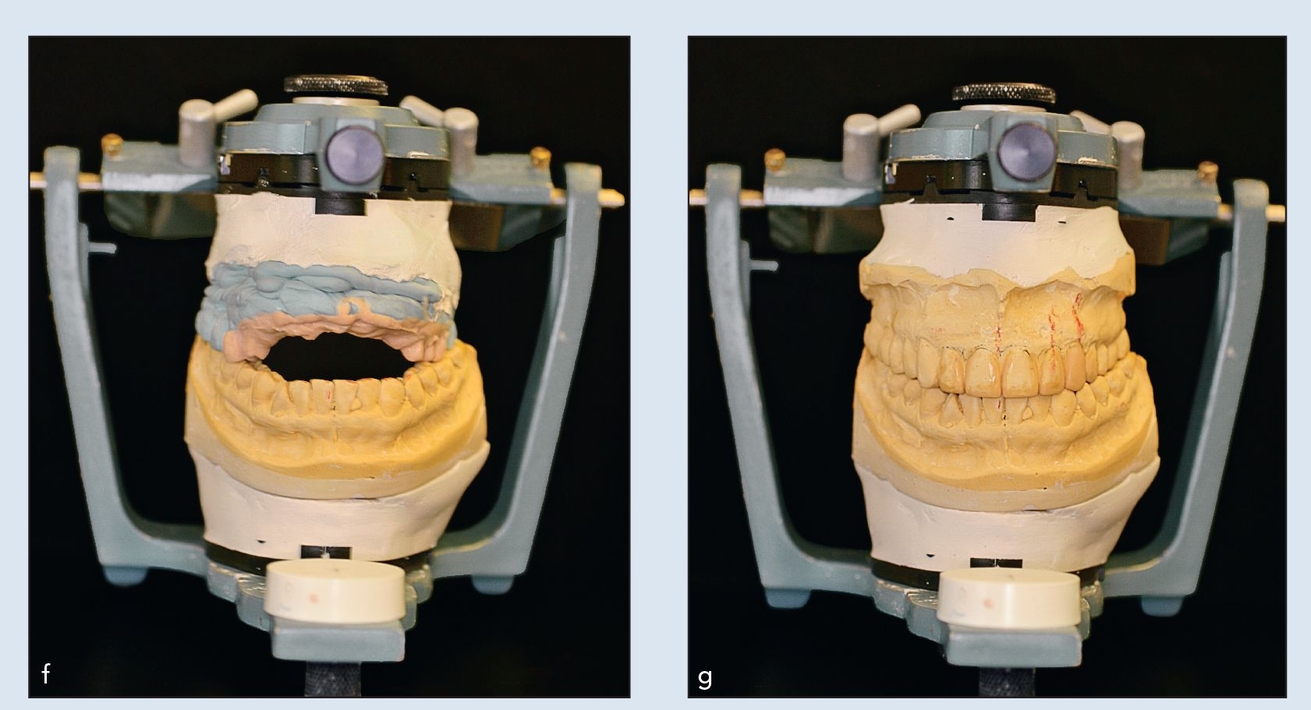
Figs 18-2f and 18-2g Mounted casts on a semiadjustable articulator utilize vertical incisor and interpupillary lines to establish a horizontal, and therefore esthetic, occlusal plane.

Fig 18-2h The diagnostic wax-up is duplicated and poured in stone to create the ECC.

Fig 18-2i A clear acrylic resin stent is vacuum formed over the definitive ECC.

Fig 18-2j Natural tooth abutments are prepared.
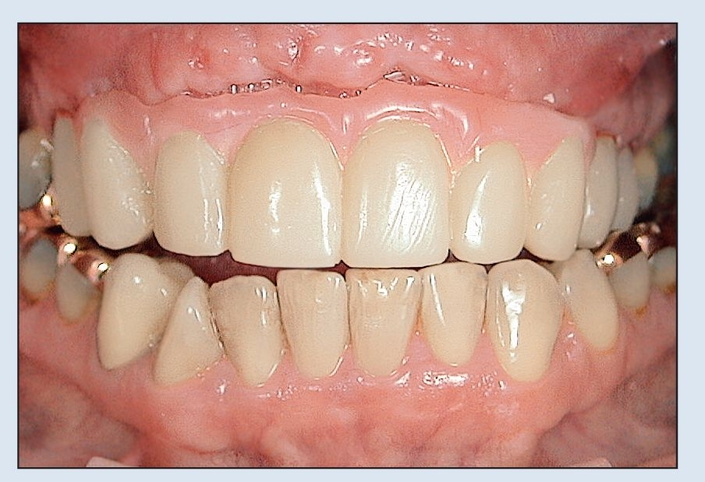
Fig 18-2k The fixed prosthesis is fitted, relined, and adjusted directly. Gingival adjustment of the pink acrylic resin may be necessary to obtain full seating of the FPP.

Fig 18-2l The FPP begins to establish esthetic parameters by broadening the smile and inclining the incisors.

Fig 18-3a Two bidirectional distractors (Mommaerts-Laster) are placed because of subperiosteal scarring and the need for additional vector control during movement of such a large segment.
Fig 18-3b The radiograph reveals the distractors in place.

Fig 18-3c The prosthesis acts as a surgical guide for alveolar positioning.

Fig 18-3d The proposed alveolar repositioning is obtained progressively (shown here at the midpoint of the distraction process).

Fig 18-3e The final position of the distracted alveolar ridge firmly engages the fixed provisional prosthesis, as established by both the surgeon and the prosthodontist.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


