Chapter 17
THE CHOICE OF OCCLUSAL MATERIALS FOR RE-RESTORATION
POSTERIOR RESTORATIONS
The material for the occlusal surfaces of the definitive restorations must be decided upon. The options are:
- Amalgam.
- Composite resin.
- Acrylic resin.
- Non-precious metals.
- Gold.
- Porcelain.
The objective of this chapter is not to assess materials according to their physical properties, but rather according to their clinical application.
| Amalgam | This is particularly suitable for interim restoration or maintenance therapy, rather than for definitive therapy for large, failed restorations. |
| Composite Resins | These materials can be used alone or with an underlying metal support. The efficacy of laboratory fabricated inlays and onlays is still uncertain and this must be borne in mind when replacing failed restorations, particularly extensive ones. It is pertinent to ask if a relatively untested material should be used when re-restoring, when a proven material is available. |
| Acrylic Resins | Acrylic resin is not durable enough for definitive therapy, but is useful during the provisional stages. |
| Non-Precious Metals | I have no experience of using non-precious metals, but from the occlusal standpoint they could be considered to have equivalent properties to gold – but being harder would be more difficult to work with. They are more difficult to solder than precious metal alloys. |
| Gold and Porcelain | The two materials most commonly used for management of the failed extensively restored dentition are gold and porcelain, they will be considered in more detail. |
Figure 17-1a shows the occlusal surfaces of an arch restored mainly with porcelain, but with gold on the occlusal surfaces of the distal abutments. The choice of material for occlusal restoration should be based not on whim or fashion, but on a logical assessment of the objectives of the restorations. These objectives relate to:
- Health.
- Function.
- Mechanical integrity.
- Aesthetics.
- Control.
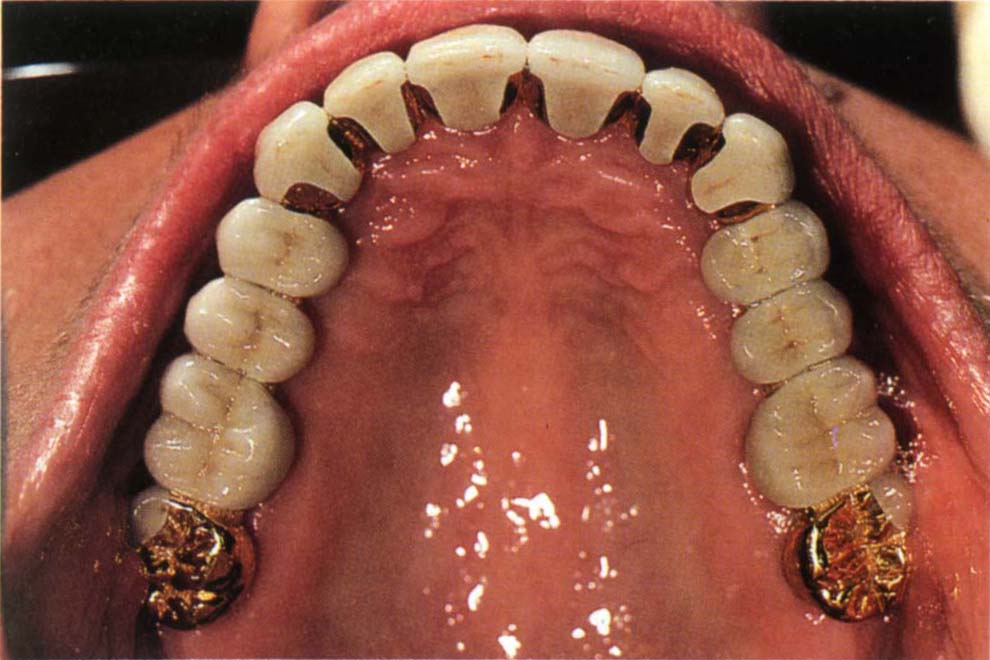
Fig. 17-1a Restoration with porcelain occlusal surfaces and gold on the most posterior tooth.
This list provides a good basis for the assessment of any restorative material. It will be discussed primarily in relation to the choice between gold and porcelain, although some consideration will be given to the other materials listed above.
Health
The objective should be to maintain the health of the following:
- Coronal tissue.
- Pulp.
- Gingivae.
- Periodontium.
- Osseointegrated fixture/bone inter-relationship.
- Neuromusculature.
Coronal Tissue
Coronal Tissue of the Prepared Tooth
There is no doubt that the minimal cast restoration, composite inlay or porcelain inlay or onlay conserves more coronal tissue than the ceramo-metal restoration, since the latter will require removal of large amounts of tissue axially. Well fitting, carefully cemented gold and ceramo-metal crowns exhibit a low frequency of secondary caries. Composite and porcelain onlays are very sensitive to technique and rely upon a hydrolytically unstable cement. The long-term microleakge effects with composite and porcelain are unknown, as is the long-term possibility of resultant caries in the remaining tooth structure.
Coronal Tissue of Opposing Tooth and Integrity of Opposing Restoration
Very little research is available to help the clinician assess the effect of the occlusal restoration on the opposing tooth. It would appear from the findings of Monasky and Taylor in 1971,1 and Locke in 1976,2 Land in 1978,3 and Fisher et al. in 19794 that the effect of glazed porcelain acting on intact opposing enamel is similar to that of enamel on enamel. Roughened porcelain has a detrimental wearing affect on the opposing enamel, while highly polished porcelain probably has a similar effect to glazed porcelain. According to Klausner et al. in 1982,5 the best way to polish the spoiled glaze of porcelain is by means of the Shofu porcelain polishing kit (Shofu Corp.).
According to Monasky and Taylor in 1971,1 porcelain occluding against gold has a detrimental effect, with progressive wear of the gold. From an in vivo study, Ekfeldt and Oilio reported in 1990 that wear rates of gold and porcelain were similar when opposing a porcelain restoration.6 A microfilled resin in similar circumstances, however, exibited approximately three to four times as much wear. It is probably advisable, wherever possible, to arrange for similar materials to oppose one another to equalize wear. It should be remembered that it is far easier to polish porcelain in the laboratory, than in the mouth following adjustment.
When striving to maintain the health of the opposing coronal tissue, easier and more predictable results can be obtained using gold on the occlusal surface of the restoration rather than porcelain. If porcelain is used, until the research shows otherwise, it should be glazed or highly polished in the laboratory, as opposed to being adjusted and polished in the mouth. The effect of composite resin on the opposing enamel has yet to be clarified. Unglazed castable ceramics have a similar effect on the opposing enamel to glazed porcelain, but glazed, stained castable ceramics are more wearing and their use is not recommended in areas in which wear could be a problem.7
Pulp
Neither gold nor porcelain have a direct affect on the pulp. However, the greater the amount of tooth removed during tooth preparation, the more danger there is to the pulp.8–10 Furthermore, the thinner the remaining circumpulpal dentine, the more likelihood of pulpal damage.11 Ceramo-metal restorations require more tooth removal than gold restorations (1.5 mm as opposed to 0.75–1.0 mm) and, therefore, are more traumatic. If one considers, for example, the dimensions of a lower first premolar as reported by Shillingburg and Grace in 1973,12 there is on average 3.24 mm enamel and dentine at the base of the occlusal fissure. Preparation for occlusal porcelain would endanger the pulp more than preparation for gold. Preparation for cervical porcelain would also endanger the pulp more than preparation for gold. The lower first premolar is particularly relevant in this context, as the occlusal surface is readily visible when the mouth is opened and could possibly be mutilated purely for aesthetical reasons, without giving due consideration to the pulp. Doyle et al., in 1990,13 recommended 10° of occlusal convergence for Dicor crowns because of pulpal anatomy; 5° weakens the crown and 15–20° jeopardizes the pulp, so that the tolerance is very small.
Gingivae
(i) Contour of the Restoration
A crown which is more bulbous than the natural crown is usually associated with an increased gingival bleeding tendency,14 indicating a greater degree of gingival inflammation. Ceramo-metal restorations are more frequently bulbous than gold restorations, as teeth are often underprepared in critical areas such as the cervical third, while technicians remove stone, representing the soft tissues, from casts so that landmarks are lost.
(ii) Joints between Restorations
A joint providing insufficient embrasure space may lead to gingival inflammation. The question that poses itself is: ‘Are the embrasure spaces more likely to be too small with gold on the occlusal surface, or porcelain?’ Consider Figure 17-1b. If these units were joined, the use of gold occlusal surfaces would enable joints to be provided at the marginal ridges, keeping the embrasure space as large as possible. If porcelain occlusals were mistakenly prescribed, the provision of 1 mm of porcelain on the occlusal surface would place the joint 1 mm closer to the gingival tissues (Fig 17-1c). If the technician uses a cast with removable dies, the soft tissues will have been removed from the cast and the technician will be unaware of the problem. Although with careful planning this could be avoided by using a metal strut which is brought up to the occlusal surface for soldering, as a general rule gold occlusal surfaces allow joints to be placed further from the gingivae than porcelain occlusal surfaces.
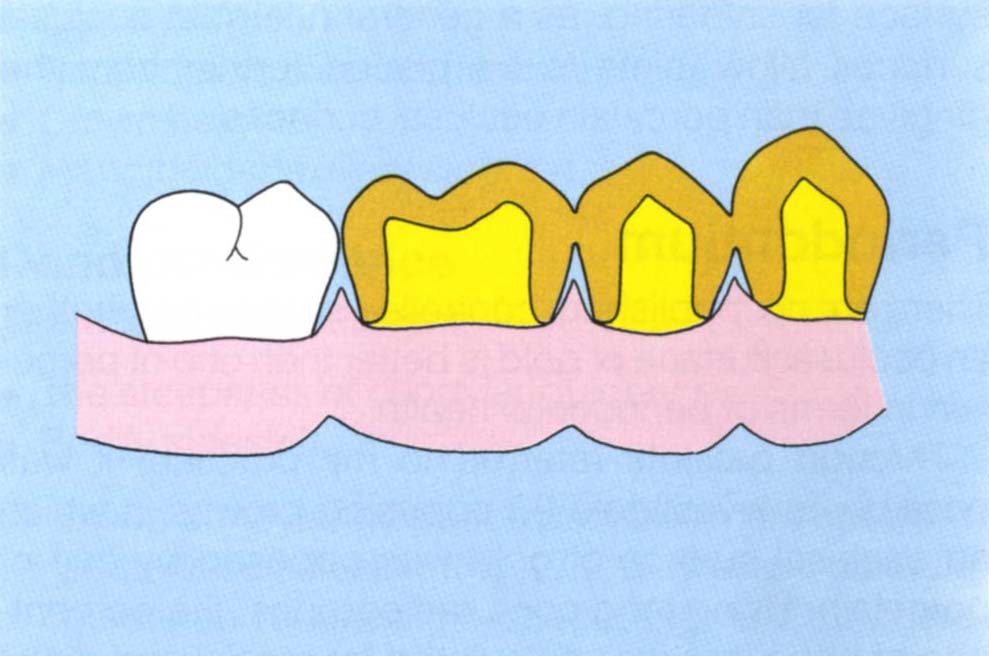
Fig. 17-1b Consider the situation if the four teeth required splinting. Gold occlusal surfaces with gold marginal ridges allows solder joints to be in their most occlusal position relative to the gingival crest.
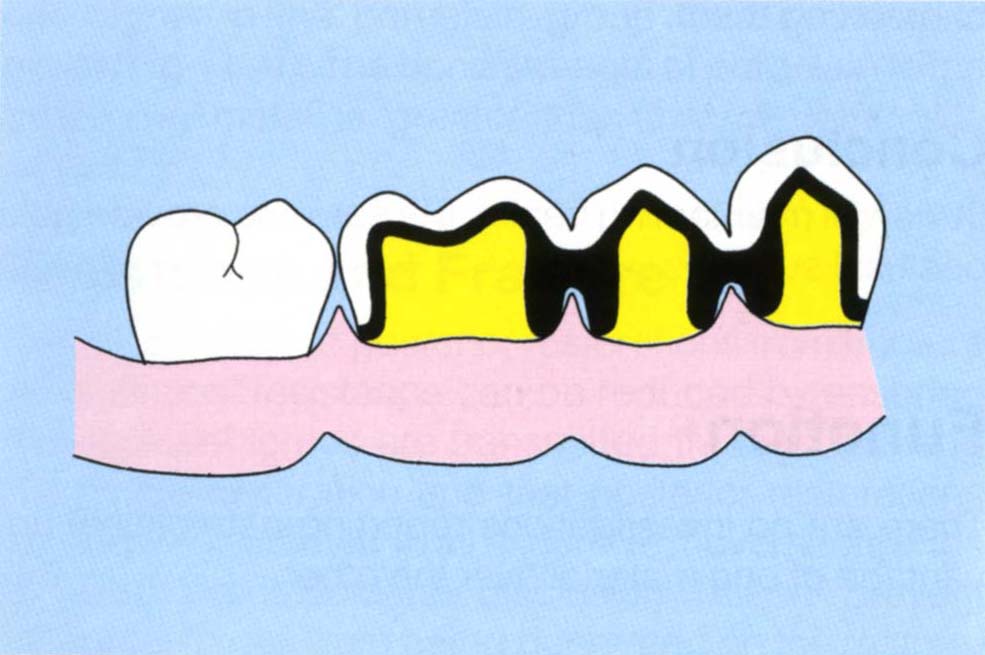
Fig. 17-1c Porcelain occlusal surfaces require the joints to move 1 mm apically as compared to gold.
Periodontium
There are no, published, controlled studies on whether an occlusal surface of gold is better than one of porcelain in terms of periodontal health.
Through patients referred to my practice, it was possible to investigate 60 opposing crowns in which an occlusal surface of gold was opposed by one of porcelain. Using long cone radiographs, the percentage of bone loss was calculated for mesial and distal surfaces measuring from the amelocemental junction to the approximal alveolar crest and to the root apex (Fig 17-1d). Reference to Figure 17-1e demonstrates no differences, in the same mouth, in the frequency of bone loss related to the two types of restoration. Obviously, these data are open to criticism, in that plaque scores are not reported, nor is it known whether bone loss had occurred before or after placement of the restorations. However, there seems no reason why the occlusal material should influence periodontal health and findings support this. Also, it should be pointed out that many of the restorations with gold occlusal surfaces had porcelain on the buccal surfaces and were, therefore, liable to be overbulbous as much as full porcelain restorations. In conclusion, therefore, there is inadequate data currently to decide whether a porcelain or gold occlusal surface is more conducive to periodontal health.
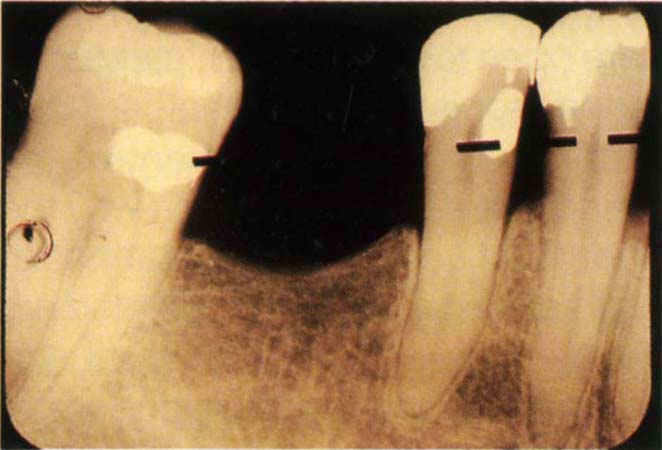
Fig. 17-1d Measurement of bone loss from long cone radiograph. Distance of amelocemental junction (broken line) to bone crest divided by amelocemental junction to apex x 100 = % bone loss. Sixty opposing teeth from 30 patients. Gold occlusal on one tooth, porcelain on the opposing tooth.
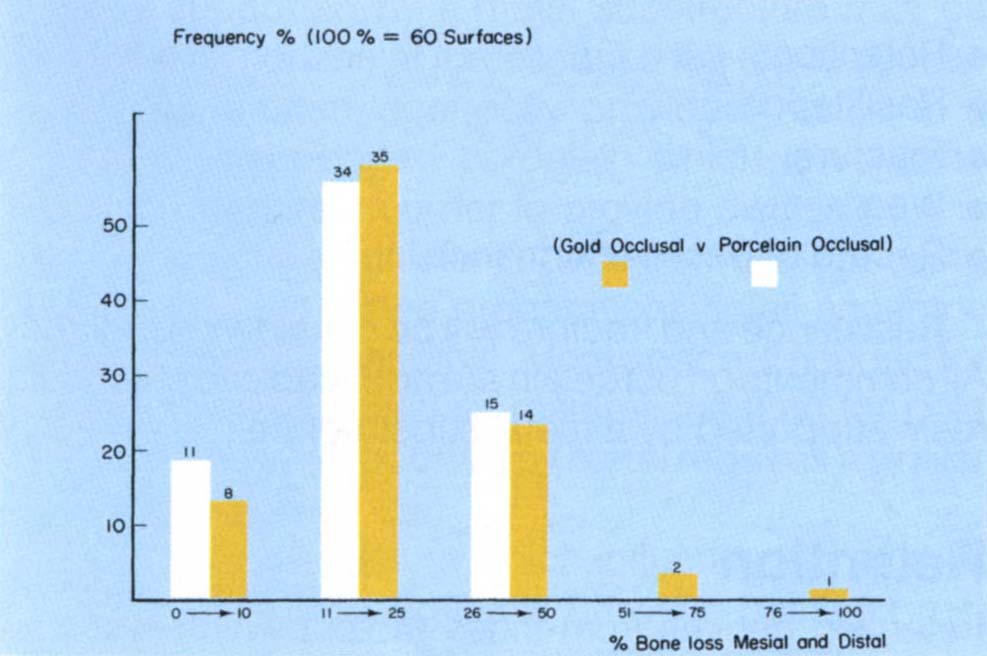
Fig. 17-1e Frequency percent of bone loss for porcelain and gold occlusal surfaces. 60 opposing crowns, 30 porcelain on one occlusal surface, opposed by 30 gold; from 30 patients in a sample of 500 patients, 60 measurements for each type – mesial + distal (Chi Square, P > 0.05 – No Significant Differences).
Osseointegrated Fixture/Bone Inter-Relationships
The consensus from the Gothenburg and Toronto schools was that acrylic resin should be used on the occlusal surfaces of fixtures and that porcelain is contraindicated. These recommendations were based upon failures observed when porcelain was used. However, Parel and Sullivan in 1990,15 described the use of porcelain on occlusal surfaces, placing great emphasis on the soldering of such bridges to obtain a passive fit of the superstructure, a requirement which all authors stress. Further, as described by Davis et al., in 1988,16 the porcelain metal superstucture provides wider stress distribution than the acrylic/metal superstructure and reduces the loading on individual abutments and retaining screws during tooth clenching. Acrylic only ‘cushions’ the abutment when biting, suddenly, on something very hard. Porcelain should be chosen when mixing osseointegrated fixture supported crowns and natural or restored teeth.
Metal supported composite resin may provide a feasible alternative in providing an aesthetic, durable, material. This choice will be further considered in Chapter 33.
Neuromusculature
It may be considered whether it is best to use gold, porcelain or composite resin on the occlusal surfaces in patients with neuromuscular problems. There is no clinical research available to enable this question to be answered. If a patient’s occlusal awareness indicates that achieving acceptable, even occlusal contacts will be difficult, then since it is easier to mark occlusal contacts on gold and to adjust them, it would seem sensible to provide gold occlusal surfaces in such cases. Furthermore, it is difficult to mark composite or porcelain inlays prior to cementation, without the risk of breaking them.
Conclusion
In view of maintaining health, it is easier to provide gold occlusal surfaces.
Function
There are no investigations reporting a functional advantage of one material over the other.
Mechanical Integrity
Five factors demand consideration:
- Retention.
- Resistance.
- Fracture.
- Wear.
- Record of past performance.
Resistance and fracture will be considered together. All comments on porcelain are applicable to composite resin supported by a metal substructure.
Retention
Retention derives from those factors which resist removal of the crown from the tooth by forces in the long axis of the preparation. Excluding auxiliary devices, such as horizontal pins, retention is provided by preparing opposing parallel walls on the preparation (Chapter 9). Since a restoration with porcelain on the occlusal surface necessitates a preparation with less occlusal height than for a gold restoration, the opposing parallel walls will be shorter for ceramo-metal restorations with porcelain occlusal surfaces than for those with gold occlusal surfaces. With short clinical crowns, therefore, restorations with porcelain occlusal surfaces will have less retention than those with gold.
Resistance
This denotes the ability of the restoration to withstand removal by forces in all directions other than axial (Chapter 9). Such forces are rotational in nature.
Fracture
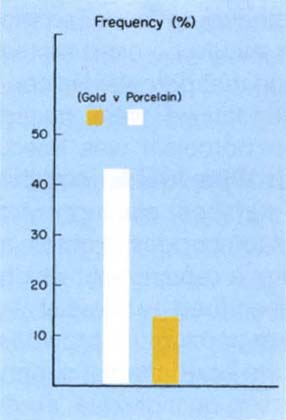
Fracture is obviously of primary concern with porcelain and composite resin restorations. Of the 30 opposing crowns reported previously, the frequency of fracture was higher in the porcelain group than in the gold group (Fig 17-1f). The bond strength of porcelain to the underlying metal is greater than that of composite resin.17–18
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


